")
-
Psychotherapeutic Fatigue
Very often my friends and acquaintances, laypeople in the psychotherapy subject, ask me if I bring my patients’ problems home along with me. Somehow, they seem to believe that psychotherapists leave their offices carrying the weight of other peoples’ problems and can hardly sleep at night.
I have always calmly answered that that is not exactly so, as therapists are required to take rigorous professional training, which enables them to distinguish their own contents from those of their patients.
That may be a good answer for laypeople , that will remain so, and also deeply amazed at our absolute skill, although a very unsatisfactory one if we really wish to reach the deep nature of this subject. Even Freud (1910: 1565), who defined the countertransference phenomenon as “an emotional answer from the therapist to his client”[1], was somewhat superficial in this analysis.
More recently, however, due to studies conducted on professional stress and violence and its traumatic sequelae, an increasing number of authors have described a kind of bio-psycho-social disease that affects those who take care of traumatized people. This “disease” is referred to in the literature by various names (Figley, 1995: 9)[2]: “Secondary Post-traumatic Stress Disorder”; “Secondary Victimization”; “Co-victimization”; “Vicarious Traumatization”; “Emotional Contagion”; “Generational Effects of Trauma”; “Savior Syndrome”; “Compassion Fatigue”; “Burnout Therapist Syndrome”, etc.
These authors’ studies do not focus on the patient or on how he may be harmed by the therapist; on the contrary, they focus on how the psychotherapist profession may be unhealthy and have a personal cost to the therapist him/herself.
There are some similarities among the different symptoms of professional stress, mainly when stress is related to excess work and bad working conditions. However, there are specific characteristics of unhealthiness occurring in the helping professions, which is the focus of this article. Being in contact with another’s trauma and trying to help traumatized people causes deep stress to the helper; ironically, the more sensitive and devoted the helper is, the more vulnerable he/she will be to the mirror-effect of another’s pain.
In this sense, I chose the terms – Secondary Post-traumatic Stress Disorder -, as in my opinion it best describes what occurs in the various psychotherapy areas, and Psychotherapist Fatigue.
WHAT IS SECONDARY POST-TRAUMATIC STRESS DISORDER?
In 1980, the Diagnostic and Statistical Manual – DSM III of the American Psychiatric Association (1989, 264-267)[3] included, for the first time, the diagnosis of Post-traumatic Stress Disorder (PTSD), to describe symptoms affecting people who go through a psychologically painful experience.
Included in this category are unusual events of human experience that represent serious threats to one’s own life or one’s children and close relatives’ life, such as natural disasters (earthquakes, accidents) or intentional disasters (torture, power abuse).
According to this manual, the trauma may be directly or indirectly experienced through learning about threats and damages to the physical integrity of friends, relatives or close people.
Thus, PTSD – Secondary Post-traumatic Stress Disorder – may be defined as natural behaviors and emotions that arise from knowing about traumatic events experienced by a significant other.
It is a process of gradual emotional exhaustion related to excessive work, and going on vacation only is not the solution; a gradual erosion of the therapist’s spirit, which involves a loss of confidence in his/her own capacity to help. Ayala[4] Pines (1993: 386-402) believes that only professionals with high ideals and motivations experience this syndrome, as if it were a strain between the professional’s need to help and the real problems involved in treating people.
Reviewing the empirical research about this syndrome, Kahill (1988)[5] identifies five categories of symptoms:
- Physical Symptoms (physical exhaustion and fatigue, sleep difficulties, somatic problems like headaches, gastrointestinal disorders, influenza, etc.)
- Emotional Symptoms (irritability, anxiety, depression, guilt, sense of helplessness)
- Behavioral symptoms (aggressive behavior, callousness, pessimism, cynicism, drug abuse)
- Professional symptoms (quitting the job, poor work performance, absenteeism, tardiness, excessive work without breaks, etc.)
- Interpersonal Symptoms (inability to concentrate, avoidance of contact with clients and colleagues, difficulties in personal life, etc.)
Duton and Rubinstein (1995: 85)[6] think that the indicators of this status reproduce in the therapist some of the symptoms of the post-traumatic stress syndrome:
- Stress Emotions including: sadness, mourning, depression, anxiety, fear and horror, rage, hatred, shame.Intrusive images of the client’s traumatic material in nightmares, for example, or in awake fantasies with visual flashes.
- Difficulty in dealing with the client’s dissociation.
- Somatic complaints such as: sleep difficulties, headaches, gastrointestinal problems and palpitation.
- Addictive and compulsive behavior including substance abuse, eating disorders and compulsive working.
- Difficulties at daily social activities and at private life roles, such as: canceling appointments, decreased use of therapy and supervision, chronic tardiness, decreased self-care and self-esteem and a sense of isolation and alienation.
- Physiological excitement.
WHO IS MOST VULNERABLE TO PTSD?
Shortly speaking, all professionals whose fundamental working tool is empathy and all people who are regularly in contact with traumatized people are potentially vulnerable to this contagious traumatization. The so called “helping” professions such as, firemen, policemen and military, emergency and rescue teams, and all professions related to health, such as nursing, medicine, especially psychology and psychiatry.
For many reasons, the last two professional categories are the most affected, from factors related to the choice of the profession to those related to peculiar working conditions.
BEING A THERAPIST: CHOICE OR FATE?
Alice Miller[7] (1997: 30-35) thinks that choosing a helping profession, especially that of psychotherapist, has more to do with fate than with choice itself. She refers to the fact that most therapists come from dysfunctional families where, from childhood, they were demanded to help, directly or indirectly, some less capable adult for that function. Ingeniously trained from childhood to be at someone’s disposal, these people have developed their empathetic ability and sensitiveness which will be their favorite working tool in the future.
Empathy, an essential tool to access the client and to plan a strategy action, makes professionals exchange places with the victims, but doing so they indirectly experience the same events that traumatized their clients. Moreover, the professional’s unresolved trauma will be revived by the report of a similar experience by the client, especially if this experience is a childhood trauma, probably due to the higher vulnerability of the child and to the remembrance of his/her own childhood.
Many authors develop studies on the characteristics of people who choose these professions. High ideals and generous hearts are some traits pointed out by Grosch and Olsen (1994: IX). They have concluded that psychology and psychiatry students constitute a group of optimistic and all-powerful young people willing not only to make money but to change the world; that after hard training along with compassion and care they will be able to transform the life of the people they are taking care of.
Freudenberg, H. (1980)[8] describes the “Type-A” personality, which comprises different traits such as high idealism and performance and low self-esteem; this kind of individuals work harder and harder in order to feel more acceptable. They are excessively devoted professionals who tend to demand too much from themselves and very often substitute social life for work. Some psychoanalysts (Allen, 1979.42,171-175) [9] believe that being successful in their careers will compensate childhood disappointments, like, for instance, unresolved fraternal rivalries or that it will represent a late Oedipal victory.
Victor C. Dias (1987: 187-195)[10] points out to the solitude of psychotherapists, who accustomed to an open and sincere communication, devoid of the usual social dissimulations and hypocrisies, end up by restricting his/her relationships to people who also communicate like him, i.e., to people who have also taken psychological therapy. This trap leads the therapist to be more and more solitary, tending to arrogance, inadequacy and social aggressiveness.
WHAT CAUSES STRESS TO THE PROFESSIONAL?
The systemic theory seeks to understand the individual through the impact that involving systems have on his/her life. The circular causality[11]concept may be applied to the therapist’s fatigue issue (see figure 1).
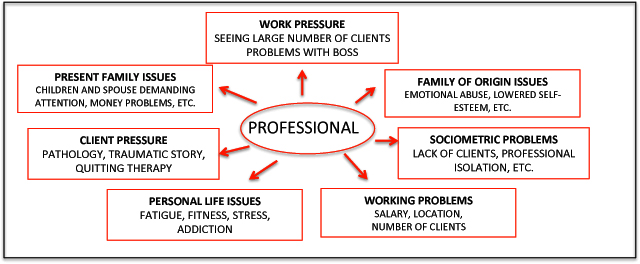
FIGURE 1: MULTI-SYSTEM PRESSURES ON THE PROFESSIONAL
This figure indicates pressures arising from various relationship systems involving the health care professional:
1-PRESENT FAMILY AND PERSONAL LIFE PRESSURE: some authors associate career success with the professional’s middle age, showing that, generally the professional attains his/her top effectiveness between 40 and 50 years of age. Also at this age, life events usually bring dissatisfaction such as: marriage crisis, aging, women’s menopause, children’s marriage, etc. Experiencing these existential crises and, at the same time, taking care of people sorely in need may be exhausting and stressing.
Grosh and Olsen (1994) conveniently describe another frequent situation to us psychotherapists: while we spend hours and hours on end listening to and being empathetic to others, we neglect our own families and ourselves. After long hours listening to patients, how many of us really feel eager to handle our children’s and companions’ routine complaints; how many of us feel like doing physical exercises or having a balanced meal? A study conducted by Michael Mahoney[12], showed that problems like overweight , sleep difficulties , a generalized exhaustion, were some of the most frequent complaints among the interviewed psychotherapists.
Sensitive heroes to our clients, we suddenly transform ourselves in careless participants of our family systems and neglectful of our own bodies.
2- FAMILY OF ORIGIN ISSUES: According to Bowen and his self-differentiation theory, people handle their family of origin difficulties with a large variety of ongoing responses from cutting their families off to completely joining them. There is no self-differentiation in any of these radical solutions. Total fusion or cutoff leaves a work to be done, which will be replied in the individual’s contemporary relationships.
The professional environment is extremely propitious to become a second family, where people play or try to play roles similar to those of their families of origin and where they expect to put an end to the former emotional drama, although they just keep repeating it.
3- CLIENT PRESSURE- In this item, in addition to the constant concern for the evolution and seriousness of the cases of which we take care, I would like to point out another professional fatigue factor.
Berkowitz (1987)[13] describes the “non-reciprocal attention” phenomenon. The author says that psychotherapists seem to be prepared to deal with others’ pain and stress, but they do not seem prepared to the patient’s lack of reciprocity. Constant giving in a one-way relationship with no feedbacks or perceivable success is hard to anyone, especially to someone who has become a therapist to understand his/her own dysfunctional roots.
The therapist’s work implies a constant “affective turn on and turn off” with the other person. Many times, at the top of a therapy process we suppose to be successful, the patient quits therapy or is abruptly withdrawn from therapy by paying parents, with no explanations; this hampers the loss and mourning process demanded by any detachment. Young therapists, mainly, feel deeply upset at these solitary losses, at the sudden divestiture of a relationship they supposed to be strong and productive.
4- WORK PRESSURE, SOCIOMETRIC PROBLEMAS, PRESSURE ARISING FROM WORKING CONDITIONS- The psychotherapy profession has some unrealistic expectations in terms of healing people in a profitable and elegant way. Unfortunately, working conditions, our consultation fees as well as our sociometry are often unsatisfactory.
Our colleagues who perform community services experience various kinds of frustration, from location and attendance to their services to the lack of remuneration. “The institution care client is the one who does not pay, often does not show up and never improves”, says a humorous quotation about the reasons to stress.
Even those who have a private office very often embitter the lack of paying clients, a low remuneration from healthcare insurers, and the self-instability of a self-employed career consequently lacking gratification from the professional life.
PROFESSIONAL ABUSE AND THERAPIST FATIGUE
The therapist’s stress may lead to a careless and abusive service to patients. Some colleagues compensate their low consultation fee by seeing many patients on the same day, or organizing excessive large groups of people, in disadvantage of work quality and of their own personal health.
The therapist’s unrealistic expectations may also affect the client’s development. The urgency to be regarded as useful and to be reassured of his/her professional ability may transform the therapist’s compassion into a pressure on the patient to perform changes in his/her life.
On the other hand, a patient’s worsening may lead the therapist to feel inefficient and frustrated. Taking Kohut’s ideas about the narcissistic issue as a starting point, William Groch and David Olsen (1994: 57)[14] describe some psychotherapists’ arrogance and “God complex”. They believe that psychotherapists who did not experience enough mirroring and empathy in their first childhood years may compensate their desire to be appreciated and esteemed using the patient for this complementary role.
In this sense, the objective of the helping careers is paradoxical: in one aspect they represent a way to transcend oneself; in another they may well serve as a means to gain others’ consideration.
Dealing with people who tend to idealize us leads to two kinds of common mistakes:
- We may assume that they are dead right, that we are really special and so we keep on doing things to maintain their opinion about us;
- We may become so anxious with this load of idealization that we’ll do anything to disappoint them – acting wrong, making stupid mistakes, or being too symmetric towards the patient.
Actually, the therapist’s role implies a certain power, which we must be prepared to assume, without excesses and for a while only. I always remember a supervisor who told me to be absent once in a while and not always replace sessions. Therapists’ faults help to adjust patients’ excessive idealization.
CONCLUSION: PREVENTION AND TREATMENT
There are many ways therapists may use to take care of their own health. All of them invariably imply a change of work and life routine. Determining the number of patients, having reasonable mealtime breaks, doing physical exercises, etc. are some of these ways, which although apparently simple, they are extremely hard to be put in practice.
It is not just a matter of working less, you must substitute a portion of the financial, professional and narcissistic assumption, which comes from a booked up agenda, for the growing awareness that we are as vulnerable as our patients and that there’s no possible way to support others’ needs if we don’t take care of our own needs.
Another desirable way is to balance clients’ attendance activities with didactic activities like giving classes, lectures or institutional work. That makes the therapist mover around, talk to other people; get into more symmetrical relationships than those he/she has with the patient.
Therapy and supervision groups are also very important, as long as they represent a safe place where the professional can expose himself without fearing reproaches and personal critics. In my point of view, a proper supervision group does not exceed 6 or 7 colleagues and implies an intimate work of constructing the professional’s role. Large groups favor idealizations and defenses that end up destroying the information originality.
Organizing small study groups on an issue jointly selected is another kind of group support that reduces professional isolation. These “groups of equals”, in addition to being productive – recycling professionals and producing written work – provide a symmetrical relationship less formal than the supervision. Almost naturally, colleagues share their working difficulties in the clinic and offer emotional control to delicate issues such as: lack of clients, sessions seemingly ill-conducted, “therapist’s love and hatred towards clients”, tips about a service that’s been worrying us, etc. Personally, I am strongly in favor of this resource.
Participating in congresses, experiences and researches on the working area also help the therapist to keep a healthy interest in his/her own personal practice.
I think it extremely important that we recognize these issues related to our professional performance and would very much appreciate it to have them discussed more often in our congresses. I believe that shame is associated to this matter, as we see each other as semi-gods, and admitting our needs might be taken for some kind of personal fault or failure.
The Greek myth of Asklepius[15], god of healing and father of medicine, gives me support to close this text:
Asklepius, son of god Apollo and mortal Coronis, was wounded before being born; his father Apollo, in a jealousy crisis upon knowing that Coronis had betrayed him, ordered her to be burnt alive. However, when he knew she was pregnant, he pulled the child from Coronis’s womb and gave it to Chiron, the Centaur, to teach him the art of healing.
Chiron, half human and half god, could never be healed from a wound caused by Hercules. Thus, Chiron, the healer, who needed to heal himself, taught Asklepius the art of healing, the ability to find seeds of light and to feel comfortable in the darkness of distress.
The paradox of the helping professions lies in the fact that the healer heals and remains wounded at the same time. All human beings have wounds and despite the excellence of our psychotherapies, they do not exclude us from our own humanity.
BIBLIOGRAPHIC NOTES
- Allen, (1979) Hidden stresses in success. Psychiatry, 42,171-175.
- Berkowitz (1987) Therapist survival: maximizing generativity and minimizing burnout. Psychotherapy in Private practice 5 (1) , 85-89.
- Dias, Victor R.C.S (1987) – Psicodrama- Teoria e Prática- Edtora Ágora -S.Paulo.
- Duton,M.A. and Rubinstein, F.(1985) – Working with People with PTSD: research implications In Figley, R.C. (1995) – Compassion Fatigue, Brunner/Mazsel, Inc, New York, U.S.A.
- Figley, R.C. (1995) – Compassion Fatigue, Brunner/Mazsel, Inc, New York, U.S.A
- Freud ,S. (1910) – El Porvenir de la Terapia Psicoanalitica- in Obras Completas , Biblioteca Nueva, 1973 ,Madrid.
- Freudenberguer, H. (1980)- Burnout: the high cost of high achievement, Doubleday Publisher, New York.
- Grosch, N. W. and Olsen, C. D. (1994) – When Helping Starts to Hurt , W. W .Norton & Company, New York, U.S.A.
- Kahill, S. (1988)- Interventions for Burnout in the helping professions: A review of empirical evidence. Canadian Journal for Counseling Review, 22 (3), 310-342
- Manual de Diagnóstico e Estatística de Distúrbios Mentais (1989) 3ª Edição -Revista DSMIII – R, Editora Manole Ltda .
- Miller, A. (1997)- The Drama of the Gifted Child, Editorial Summus, S.Paulo.
- Pines, Ayala (1993)- Burnout: Handbook of Stress. Free press.. Psychotherapy in Private practice 5 (1) , 85-89 , New York:
- A. (1999)- Aesculapius: A Modern Tale- MSJAMA online: http://www.ama-assn.org/sci-pubs/msjama/articles/vol_281/no_5/jms90003.htm
[1] Freud ,S (1910) – El Porvenir de la Terapia Psicoanalitica”
[2] Figley,R.C.(1995) – Compassion Fatigue
[3] Manual de Diagnóstico e Estatística de Distúrbios Mentais , 3ª Edição -Revista DSMIII -R, Editora Manole Ltda 1989 pp . 264- 267
[4] Pines, Ayala- Burnout-Handbook Of Stress
[5] Kahill, S. (1988)- Interventions for Burnout in the helping professions : A review of empirical evidence. Canadian Journal for Counseling Review, 22 (3)3310-342
[6] Duton,M.A. and Rubinstein, F.- Working with People with PTSD: research implications
[7] Miller, A. (1997)- O Drama da Criança bem dotada
[8] Freudenberguer,H. (1980)- Burnout: the high cost of high achievement
[9] Allen,1979. Hidden stresses in success. Psychiatry ,42,171-175
[10] Dias,Victor, R.C.S. ( 1987) Psicodrama-Teoria ePrática
[11] Circular causality: everyone is related in the system, therefore any change affects all individuals and the system as a whole
[12] Mahoney, Michael – Personal Communication in a workshop on “”The personal life of the psychotherapist”. He is a MD, PhD – from Stanford University, author of various books on the Cognitive and Constructivism approach.
[13] Berkowitz(1987)-Therapist survival: maximizing generativity and minimizing burnout. Psychotherapy in Private practice %(1) , 85-89
[14] Willian Groch e David Olsen (1994)- When Helping starts to hurt
[15] Stanton, J.ª ( 1999) – Aesculapius: A modern Tale
-
FOUNDATIONS OF PSYCHODRAMA: THE IMPORTANCE OF DRAMATIZATION
The other day, one of my colleagues of “GEM” – Moreno’s study group – said something very curious about round tables in congresses. She said that no matter what the table theme is, the debaters always talk about what they like, i.e., they take the opportunity to make public the points of their own interest, not necessarily the ones proposed by the organizers.
I normally follow rules, but when I considered this table theme – Foundations of Psychodrama – it soon came to my mind two ways of approaching it: in the first, I would interpret the word ‘foundation’ as a solid basis that legitimates and authorizes the psychodramatic practice; in the second, I would seek what seems to me to be fundamental, essential and indispensable to Psychodrama.
I confess that I was more attracted by the second possibility, as for Moreno (1999:33) Psychodrama is just one of the methods of sociatry, one of the three components of socionomy: sociodynamics, sociometry and sociatry. (figure 1)
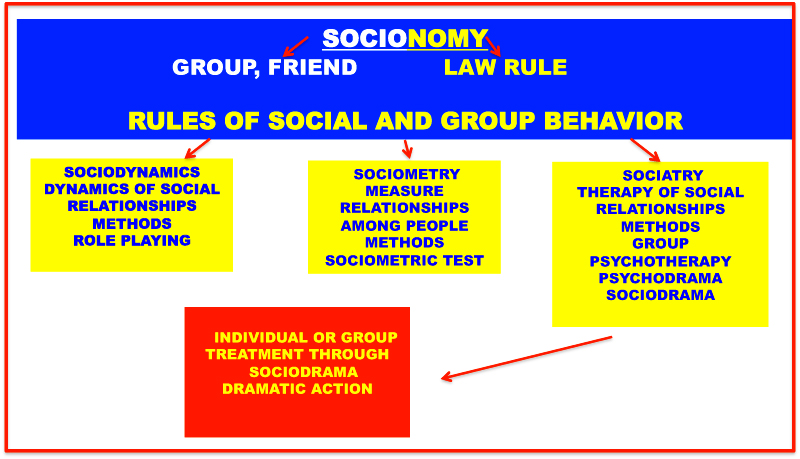 FIGURE 1 – SOCIONOMY
FIGURE 1 – SOCIONOMYSearching for the foundations of Psychodrama would involve establishing the basis for the whole of socionomy, i.e., describing the foundations of all of Moreno’s work. At least, I would have to mention the Morenean vision of the spontaneous man, his philosophy of the moment, as well as his Role Theory and Action Theory. Honestly, I would not be able to do that in 15 minutes.
Therefore, I chose the second possibility, i.e., to understand the word ‘foundation’ as what I consider to be the basic, essential and indispensable attribute to Psychodrama .
Moreno describes Psychodrama in many ways. In one of them he defines Psychodrama as the treatment of an individual or group through dramatic action (1992:183).
Personally, I consider the dramatic action one of the fundamental characteristics of Psychodrama and its absence concerns me, especially in relation to the bipersonal status. Many colleagues, who are teachers-supervisors, say that they do not like and do not dramatize in the absence of an auxiliary-ego or supplied with objects and cushions. I must point out that I do not doubt the efficiency of psychodrama without drama, as I know that the success of a treatment does not lie in one factor only.
What amazes me is that some colleagues do not consider such a fantastic technical tool as dramatization, which therapeutic value has been more and more experimentally proven. Therefore, in the next 15 minutes, I would like to comment on three therapeutic aspects of the dramatic action that seem fundamental to me:
1- IT PROVIDES A MUSCULAR ENERGETIC DISCHARGE, NECESSARY FOR PATIENTS TRAUMATIZED BY VARIOUS CHILD ABUSES OR CARRYING TRAUMA
SEQUELAE OF ACCIDENTS (POST-TRAUMATIC STRESS DISORDERS).
Studies on trauma and its long-lasting effects in people’s lives have proved that Moreno (1959, p.239) was right to say that “act hunger” is a human physiological need just like eating, drinking and breathing.
The immediate response to a stressing situation** releases mechanics of the sympathetic nervous system reaction, known as “alert reaction”. When the animal organism gets ready to fight or escape, its breathing becomes deeper, the blood flows from the stomach and intestines to the heart and to the muscles; the ongoing processes in the alimentary canal cease, sugar is released from the liver’s reserves, the spleen shrinks and releases its contents, the hypothesis stimulates the adrenal glands and the body is flooded with hormones, like adrenaline. That’s an efficient preparation for activity and combat, as Walter Cannon had described, in 1939, and Paul MacLean reaffirmed, in 1952.
Studies developed on the animal kingdom (Levine, 1999) show that when an animal is hindered from reacting, archaic brain mechanics start operating, i.e., the reptilian brain, provoking freezing of the vital functions, thus simulating death. Through this trickery, the animal succeeds to be left by the predator or at least, to gain time to think of another escape strategy.
The same occurs, with some differences, to the human animal. In 1952, the American neurologist Paul MacLean described the triune theory of the human brain, a result of our phylogenetic evolution (See figure 2).
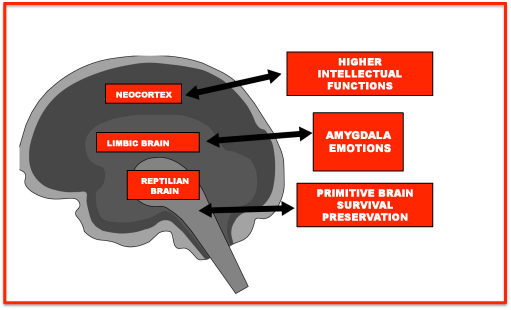
FIGURE 2. PAUL MACLEAN “THE VISCERAL BRAIN” (1952)
The brain stem is the primitive, reptilian brain, a remnant of our prehistoric past.
It is useful for quick decisions that do not demand much thinking. The reptilian brain focuses on survival; it is fear-driven and takes over whenever we are in danger and do not have time to think. In a world where the fittest survive, the reptilian brain is concerned with getting food and not with becoming food.
The central part of the brain is the limbic part or mammalian brain, the root of emotions, humor and feelings. The neocortex is the most evolutionary advanced part of the brain. It controls our ability to speak, think and solve problems. The neocortex affects creativity and the ability to learn, comprising approximately 80 per cent of the brain.
As we can see, the human brain is more specific. However, as Le Doux and Van Der Kolk (1996) demonstrated, the brain is not fully functional in traumatic situations, as the neocortex undergoes functional alterations releasing hormones that make it numb. (figure 3).
The memories filed at this moment do not need to be verbalized, they are formed by sensations, visual images and motor patterns, as language is a neocortical function.
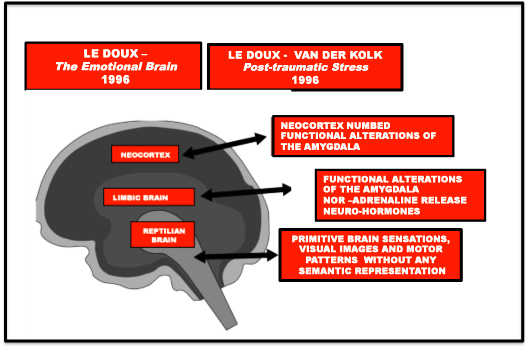 FIGURE 3- BRAIN FUNCTIONING IN POST-TRAUMATIC STRESS
FIGURE 3- BRAIN FUNCTIONING IN POST-TRAUMATIC STRESSLike the animal, the human being when prevented from reacting, functions with the reptilian brain. Freezing of vital functions is shown through superficial breathing and stiff muscles, simulating “rigor mortis” and anesthetized mind, as in an ethereal state. But contrary to the animal, which after the danger is past defrosts through a noticeable body shivering, the human being mingles these physical functions with thoughts, feelings, emotions, invisible loyalties, etc¾ which are results from the other two parts of the brain.
Many times, a person who was raped, for example, conceals his/her horror, refrains from crying, shaking and feeling ashamed to pretend that nothing’s happened. As a result of this non-action, his/her body will not recover from the trauma and the helplessness feelings experienced at the moment he/she was attacked. The individual lacks an offensive action and control recovery, which often are only attained many years later, through the active repetition of violence or abuse, this time taking the role of the abuser or of someone who holds control (many addictions are disastrous attempts to simulate control).
Dramatization allows this missing action to come about, enabling muscles to produce a safe discharge of the body’s need for control recovery. I would like to remind you that psychodrama was one of the first body therapies; Moreno said that the body remembers what the mind forgets, especially events that take place in early childhood, even before language acquisition. The best way to recover the memory of actions is through expressive methods, which address the whole person (body and mind) in the action.
2- IT PROVIDES ACTIVE AND RESPONSIBLE RESEARCH OF THE PATIENT IN RELATION TO HIS PROBLEM
As I described above, hindering of an offensive reaction creates a lethargic and helpless attitude before reality. Needless to say that most of our patients feel like this towards their own lives. They feel that something must be changed, but they don’t feel capable of undertaking this change.
In many talk therapies, especially when interpretation is utilized, the key to the symbolic puzzle, to the meaning of feelings and thoughts, to how they relate to the past, present and future seems to be in the therapist’s hand. The patient is just the patient ¾ he/she expects the therapist to do his job. This only reinforces his/her already known fragility and helplessness.
Bustos has a small picture in his office that says: “what they say about me that was not disclosed by me does not fit me”; Milton Erickson (1983, pp. 45), the innovative American psychotherapist, father of modern hypnotherapy and whose methods inspired the systemic, strategic, familiar therapies, etc ¾ also thought that the direct interpretation of the therapist represents raping to the unconscious of the patient, who releases a host of defenses to dissociate, deny, i.e., to defend himself as much as he can. We penetrate indirectly into the patient’s unconscious, through the back door, with much warming-up, and never ahead of the patient himself.
Moreover, all patients have a sound and combative portion and I particularly make my patients aware of this from day one. I always ask them what they feel like working with in that specific session and I have them play the situations they choose to work. They are active researchers like me. Decoding their material, their emotions, decisions, etc, is our joint task, often their task more than mine.
3- IT OFFERS THE SURPRISE ELEMENT TO A PATIENT ACCUSTOMED TO FUNCTIONING WITH DEFENSIVE MECHANISMS ONLY.
Dramatization has no predetermined script. I never know what is going to happen, much less does my client. I am often amazed at what comes up and I love to see my patients’ surprised look. I surprise them too, playing roles and counter-roles unexpectedly, seeking an interpolation of resistances very useful to stimulate spontaneous-creative answers, i.e., new answers to old situations.
Moreno (1923, p. 54) already mentioned the surprise function in the activation of spontaneous-creative processes. In turn, Milton Erickson (1983, p. 50) used the confusion technique to induce to hypnosis. For example, he would ask a person to imagine him/herself climbing into an airplane flying to the USA and at the end of the trip, after various commands, he would ask the person to find him/herself landing in India. He knew that the surprise tactic unbalances the intrapsychic defenses, compelling the mind to produce a different responsive energy.
The surprise element is also present in childhood traumatic situations or even in accidental traumatic situations, compelling the patient to create a defense that will give him back a feeling of control. Healing provided by dramatization is somehow driven by the homeopathic principle of prescribing the same factor that caused the disease, with the objective to heal it.
I can’t think of anything more anti-morenean than a therapist listening and interpreting his/her patient verbally. It would at least require triggering an internal action in the patient according to internal psychodrama or Fonseca’s relation therapy, doing reverse roles sat down or symbolically favoring his/her amazement and surprise, although without the benefit of muscular associations provided by body movements.
Finally, I would like to say that I believe the lack of dramatization in many psychodrama sessions is due to the unawareness of how and why to dramatize rather than to the difficulty of doing it without auxiliary egos or a group.
Supervising my students, I came to the following list of more frequent questions regarding dramatization:
- How to handle issues related to therapeutic relationship: contract (timetable, location, fee, repositions); patients who do not wish to undergo dramatization, etc.
- What is the objective of dramatization? Is the objective exploratory (like a social atom), experimental (training of roles), or does it aim to repair narcissistic damages? (dramatization of childhood scenes)
- How to choose a scene to be dramatized? How to choose a scene when the patient is too talkative? Who should choose the scene: the therapist or the patient?
- How to establish time in dramatization, i.e., present, past and future? How to go from the present complaint of the patient to the past (regressive scene), or to the future (feared and desired scenes) and then come back to the here and now in the relationship with the therapist?
- How to warm up the patient and keep this warming up throughout the dramatization?
- How to decide which technique to use, among the classical ones?
- Which is best: an open scene psychodrama or an internal psychodrama?
- How not to get lost in the middle of a dramatization session?
- What to do when session’s time is over in the middle of a dramatization session?
- How to finish a dramatization?
As you may conclude, my colleague, the one who says that no matter what the table theme is the debater always talks about what he likes, was right.
I really believe dramatization to be one of the most important tools for psychodrama and I think that better prepared students regarding these topics have less fear to use dramatization and may realize the advantages of using action techniques to help their patients.
Thank you very much.
Rosa Cukier
BIBLIOGRAPHIC NOTES
- Cukier, Rosa (1992) – Bipersonal Psychodrama, its technique, its patient and its therapist, Editora Àgora, S.Paulo.
- Cannon Walter (1939) – The Wisdom of the Body, Nova York, Norton, Quoted by Anne Ancelin Schutzenberger – “Querer Sarar”, Editora Vozes, Rio de Janeiro, 1995.
- Lê Doux, Joseph.(1996) –The Emotional Brain, Editora Objetiva, Rio de Janeiro
- Levine P.A. (1999) – Waking the Tiger – Healing Trauma – Editora Summus, S. Paulo.
- Moreno, J. L (1923). – The Theater of Spontaneity. São Paulo: Summus Editorial, Ltda, 1973
- Moreno, J. L. (1959) – Group Psychotherapy and Psychodrama, Editora-Livro Pleno Ltda., Campinas,1999.
- Van der Kolk, B. Mc. Farlane A. Weisaeth L. (eds.). Traumatic Stress: the effects of overwhelming experience on mind body and society. New York, Guilford Press. 1996
- Zeig, K. J. (1983)- Didactic Seminars on Psychoanalysis by Milton H. Erickson, Editora Imago, Rio de Janeiro
- ** Stressing situation means any situation leading the individual to a state of despair, either for striving to preserve his/her life or the life of a significant other.
-
CODEPENDENCE– do you know anyone who suffers from this disorder?
Someone once jokingly said that the difference between human beings and animals is not so much to do with being rational, but rather to do with the fact that humans have relatives. Perhaps due to the fact of being born “semi-prepared” and having a long childhood in the care of someone who has helped them survive, human beings are animals who engage longer and more in-depth with their predecessors and successors.
Father, mother, brothers and sisters, grandparents, parents-in-law, uncles, aunties and cousins…….. this makes us completely unique and is also the source of our biggest problems!
This is the case of codependence, a type of emotional and bonding pathology, described by human behaviour experts in the USA. The first studies date back to 1983, and despite not yet being classified in the DSM-IV, various books1 have been written on this topic including one already translated into Portuguese.
At first, the description of this disorder included only families of alcoholic patients, but over time its meaning has been understood in a broader context and currently the term “codependence” also refers to the conduct of families and relatives of people who have some kind of serious, chronic, physical or emotional problem.
“A codependent person is someone who lets the behavior of another person control his/hers and who is, in turn obsessed with controlling the behavior of the other person.”
Everything begins with the fact of finding ourselves connected (because of love, obligation or duty) to someone who is very complicated, physically or emotionally ill, and owing to this illness self destroys or no longer wants to live, and apparently needs our support and constant care.
This person could be a child who was born handicap , an adult suffering from depression, a wife or lover who has anorexia, a brother who did not do well in life, a sister who is always getting into trouble and seems to be too fragile to solve her own problems or an alcoholic father. To sum up, the important thing is not who this person is or what illness they have.
The core of the issue is in ourselves, in how we let this person affect our behavior and the ways we try to influence their behavior or “help them”.
I am talking about a reaction to someone else´s self destruction who ends up destroying us. We become victims of other people´s illnesses and the more we try to make this person give up their addiction or change their attitude to life, the less they get better and the more devastated we become.
It seems like our life revolves around them. We do not act on our own accord, but rather we react to how the patient is: if they are well, we are well, we make plans, we are hopeful; when they turn to drinking or get depressed, we put off going to the cinema, doing things and we feel terrible.
I know that many of you already know what I am talking about because you have probably experienced this or attend people who have experienced similar situations. Perhaps what you are not aware of is that some scientists consider this behaviour of chronic help to the other in itself an emotional, serious and progressive disorder. They even say that the codependent wants and looks for complicated people to connect with and can only be happy this way.
I do not think exactly the same way, as many codependents that I have attended were people who were tired of suffering and who really wanted to change, but whether due to upbringing, religion, guilt…. every case is a case -, they were not able to disconnect.
Some common characteristics codependents have called my attention: they are usually people who have a generous nature, they come from emotionally disturbed families and ever since their childhood have wanted to fix things that were wrong; they tend to make themselves responsible and guilty for everything; they very much depend on love, praising, and other people´s evaluations; they think they know best and can deal with certain situations better than others; they lie to themselves saying that “things will get better tomorrow”; “this is the last time” …; they doubt whether they will be happy in the future or if one day they will find true love; they find it difficult to get close to people, have fun and be spontaneous; they alternate over-affectionate care for a person who is ill with aggressive and rude ways of dealing with them; as time passes they feel ever increasingly unhappy, depressed, isolated and violent; they have eating disorders (either eating too much or too little); they end up having some kind of addiction: cigarettes, alcohol, tranquilizers, etc.
Generically, this illness is associated to various forms of child sexual abuse and codependents basically have difficulties in five areas: 1 – low self esteem; 2 – difficulty in setting boundaries; 3 – difficulty in recognizing and assuming their own reality; 4 – difficulty in taking care of their needs as an adult; 5 – difficulty in expressing their emotions moderately.
Is there any cure for codependence? There is no simple answer to this question. In the USA, self-help groups have been set up, such as alcoholics anonymous groups for families, where they try to discuss and offer support to codependents.
My own experience has shown that psychotherapy, especially psychodrama which is an approach that favors the study of bonding, is often very useful in cases where the codependent is disillusioned by their own potential to change the other person´s life and begins to really want to change their own life. The treatment helps and encourages the patient to undertake the necessary changes, to face their abusive past and to change their attitude concerning their ill relative so that they can live more healthily again, even if the relative still wants to die.
Bibliography
- Beattie,Mellody ( 1994) – Codependência nunca mais! – Editora Best Sellers, São Paulo.
- Rosa Cukier (1998)- Emotional Survival: from the child wound to the adult drama, 2007, Lulu publisher.
- Cermak,T.L (1986) .- Diagnostic criteria for Codependency- Journal Of Psychoactive Drugs. 18(1):15-20 citado por Mellody , Pia.- Facing Codependence, Harper & Row, Publishers, San Francisco ,1989.
- Mellody , Pia ( 1989)- Facing Codependence, Harper & Row, Publishers, San Francisco .
-
I HATE YOU . . . PLEASE DON’T LEAVE ME!:THE BORDERLINE CLIENT AND PSYCHODRAMA
Perhaps some therapists have already had the experience of working with a client who becomes furious during the session, complaining about your ability as a professional, about something that was said or even the way it was done. In general, we therapists become very unsure of ourselves at these moments. We do not know how to act, on the one hand trying to find out what we did incorrectly and on the other being absolutely sure that it was more the client’s performance, which then causes us to be angry and sometimes afraid of him.
As therapists, we know it is not easy to admit that we may feel anger and fear toward our clients. However, in the specific case of the borderline client, these are the exact feelings that he commonly produces in the people who are the most intimate and dear to him. Therefore, it is essential that the therapist know this and decodify his own emotions without blame or shame, so as not to act in a complementary way and to be able to help the client understand the psychodynamic involved in the process.
Lineham (1993:3) estimates that 11% of the non-committed psychiatric clients, and 19% of the committed ones in the United States are borderline clients. Among those who are diagnosed with “personality disorders”, 33% of non-committed clients and 63% of committed ones are considered to be borderlines. This type of client is, therefore, frequent enough for one to believe that all therapists, in general, have had at least one case. Besides this, they are also the ones who most commit suicide. It is estimated that 70 to 75% of borderline clients have at least one self-destructive episode or act, with approximately 9% of the cases being fatal (Lineham, 1993:3).
In Brazil, we do not know of any work concerning the prevalence of this pathology within mental diseases. However, considering our own clinics and the experiences of co-workers, we think that something similar must be taking place. What is intriguing is that besides the great danger of this condition, the available therapies fail without exception, and therapeutic advances are extremely insignificant and slow. The clients normally come to the clinics with a list of therapists whom they have already consulted, over medicated (as doctors try several psychiatric medicines to control the symptoms), and their families seem devastated and with no hope of attaining proper help.
BORDERLINE PERSONALITY CONCEPT 3
The term “borderline” was used for the first time by Adolf Stern in 1938 to describe a group of clients who appeared not to be benefiting from classical psychoanalysis, and who did not fit in the “neurotic” or “psychotic” categories. In reality, according to his classification they had a type of borderline neurosis.
In 1980, the condition was included in the Diagnosis and Statistics Manual – DSM III of the American Psychiatric Association4 which initially listed eight criteria (in the following revision, nine), five of which must be present to make the diagnosis of borderline disturbance:
1-Pattern of unstable and intense interpersonal relationships, characterized by alternating between idealization and devaluation extremes.
The borderline client thinks in a dichotomous and radical way. His world, like the child’s, is full of heroes and villains, and not infrequently any slip-up or failure by the hero inevitably condemns him. He does not understand gray areas, inconsistencies or ambiguities. Good and evil do not mix: somebody is either totally good or totally evil. He idealizes and is disappointed all the time, appearing to be eternally searching for the perfect caregiver, the one who will always be correct.
2-Impulsiveness in at least two areas5 potentially harmful to himself. (waste of money, sex, drug use, shoplifting, reckless driving, episodes of voracity).
The borderline lacks the ability to postpone gratification: his behavior results from intense momentary feelings and does not seem to learn from experience. He has an altered notion of time: “yesterday” and “tomorrow” are meaningless; only “today” seems to exist.
3-Instability in showing affection due to accentuated mood reactiveness. (episodes of intense dysphoria, irritability, or anxiety usually lasting a few hours but rarely more than a few days).
The borderline client’s mood can vary greatly in only one day or even in a few hours. He is not usually calm and controlled but frequently hyperactive, pessimistic, and depressed. His reactions are generally very intense and inappropriate for the situation that produced them.
4-Intense and inappropriate anger or difficulty in controlling it. (Frequently demonstrates irritation, constant anger, and reoccurring physical fights).
His fits of rage are unpredictable and disproportionate to the frustrations that produced them. Domestic scenes of the type: screaming, breaking objects, threatening with knives, and hitting/scratching people are typical of these clients. The anger appears after any trivial offense, but in reality seems to come from some underground arsenal, from the fear of being abandoned or disappointed.
The borderline’s anger is directed at those closest: relatives, therapists or doctors. It aims to test the bonds and commitments in an incessant search to find out how far he can push people. It seems to be an incompetent cry for help, as it ends up pushing away the people whom he needs most. For this reason, many therapists stop the treatment early or limit the number of borderline clients whom they treat.
5-Threats, gestures, or recurring suicidal and self-mutilating behavior.
This self-destructive behavior has a double meaning: firstly, it is witness to the depression and despair underlying these conditions: to feel physical pain is, in extreme cases, the only way of feeling alive and/or a very efficient way of distracting oneself from greater suffering; secondly, the para-suicidal6 behavior shows these client’s need to manipulate the people who take care of them in order to get more attention or love. In general, they do not want to die but only to communicate their suffering in a convincing way.Paradoxically, because of being insistent and repetitive they end up driving people away, which makes them needier, more desperate, and with a greater desire to hurt themselves.
Many clients report feeling calm and relieved after such “accidents”, and some scientists try to explain this phenomenon attributing it to the release of endorphins, which are a kind of self-treatment by the organism when in pain. Effectively, both self-destructive behavior as well as the well being it leads to are not easily understood phenomena.
In relation to psychotherapy, this symptom is what causes therapists their greatest problems: they pay a great amount of attention to these behaviors, running the risk of reinforcing them; on the other hand if they are ignored, the client can insist and go on in a progression of attempts to cause a stronger impact, which can result in suicide.
Self-mutilation, except when associated with psychosis, is a type of borderline disturbance trademark. There are many different ways for a person to self inflict harm: he can cut himself, smoke or eat in excess, obviously neglect his body, drive recklessly, etc.
6- Identity disturbance; accentuated instability and resistance to self-image or the feeling of self.
The borderline person lacks a clear perception of the limits between himself and the other. In general, he needs to impress people to keep them around him, and his sense of identity and self-esteem are associated with getting this attention or not. Therefore, he has to always be proving this, but deep down he has a feeling of non-authenticity, of falseness. Even when he achieves success, the borderline gets upset, believing that he did not deserve it or that at any time they will find out he is a fraud and will be humiliated.
That is why these people go from job to job, not sticking to any of them: they always have the hope that the next one will be different and they will feel better there. Literally, they cannot “find themselves”. Many times questions of sexual identity are also included in this confusion, since in the same way that the borderline does not know whom he is, he is also not able to decide what he desires.
7-Chronic feeling of emptiness or boredom.
The absence of a strong sense of identity must culminate in a feeling of existential emptiness. This is so painful that the borderline searches out impulsive and self-destructive behaviors to get rid of this sensation.
8-Frenetic efforts to avoid real or imaginary abandonment.
In the same way that a child is not able to distinguish between the occasional absence of his mother or her death or disappearance, the borderline experiences occasional loneliness as a sensation of complete and eternal isolation.
He cannot tolerate loneliness, becoming gravely depressed with real or imaginary abandonment as he loses the sensation of being alive. His existential motto appears to be: “if others interact with me, than I exist.”
9-Transitory paranoid ideation related to stressful situations or severe dissociative symptoms.
In high stress situations, the borderline can show temporary dissociations, confused and delirious thinking, and paranoid interpretation of the facts. In general, he presents himself as a victim of an unjust situation.
DIFFERENTIAL DIAGNOSIS
The differential diagnosis between the various personality disturbances is not an easy task, as mixed conditions with similar symptomatology are common. In reality, the borderline disturbance is compatible with various other pathologies, making it difficult to know what came before – for example, if the personality disturbance came before a period of depression or alcoholism or if it were secondary to these occurrences.
Many times the borderline client presents a paranoid and split ideation, only differentiating himself from paranoid schizophrenic clients because the crises are faster and do not cause acute after effects like in schizophrenia. Besides this, the schizophrenic ends up getting used to his deliriums and persecutions, being less disturbed by them than the borderline.
In relation to diseases of intimacy, mainly bipolar ones, there are similarities relative to sudden changes of mood. However, in the borderline these changes are faster and, even in the period between crisis, he has difficulty in adapting to reality. It is also possible to confuse a borderline with a chronic hypochondriac, as they both maintain intense physical complaints to achieve bonds of dependence with family members and/or doctors.
Many authors still believe that there is a high prevalence of borderline disturbance between clients who are diagnosed with multiple personalities or post-traumatic stress.
Herman (1992:123-129) studies survivors from various types of trauma (such as varied forms of child abuse, rape, war, etc.) suggesting the generic name of “Complex Post-Traumatic Stress Syndrome” to include all these conditions. She correctly argues that the “borderline personality” diagnosis has caused more damage than benefit for the study of personality disturbances. Like the term “hysterical” whose negative and pejorative connotation ended up becoming psychiatric jargon, the word “borderline” has come to mean manipulator and troublemaker over the last few years. This makes it impossible for the clients to be viewed as heroic survivors of severe childhood drama, with all the respect that this fact requires. This author also shows that the psyche has and uses some defensive resources against limiting- situations that make an attempt against human dignity. Dissociation, intrusion, irritability, self-hypnosis, impulsiveness, intense mood swings, self-mutilation, etc. are some of the defensive tools that will later constitute the different conditions of personality disorders.
Another dysfunction that is often associated with the borderline personality is the narcissistic personality disturbance. It is especially noteworthy because of the presence of a hypersensitivity to criticism and that any failure can cause grave depression. The great difference here is that in the long term the narcissist ends up being, in general, professionally successful. He works very hard to construct and keep up his powerful public image, being deeply self-centered and not getting personally involved with others. The borderline, on the other hand, does not have staying power or discipline and destroys bonds of affection and professionalism. Besides this he is sleazy, insistent, and very vulnerable to others’ opinions.
As far as the diagnostic similarity to clients categorized as para-suicidal in the AXIS and DSM diagnostic manuals, there are in fact symptoms common to both conditions such as: accentuated emotional loss of control, irritability and hostility, serious interpersonal problems, patterns of behavioral loss of control, drug abuse, sexual promiscuity, and previous suicide attempts. The cognitive difficulties are also similar: stressed cognitive rigidity, dichotomous thought, little capacity for abstraction and problem resolution. Such cognitive difficulties are related to the episodic memory deficit. The individuals affirm that their behavior is to escape an unbearable life.
It seems certain that the behavior that most differentiates the borderline from other conditions of personality disturbance is the presence of self-destructive acts and suicide attempts. Among those who show the eight DSM-III-R criteria, 36% kill themselves, compared to 7% of those who show five to seven of these criteria.
ETIOLOGY
Three types of causes come to mind when one tries to explain this disturbance: inappropriate emotional development, and constitutional and sociocultural factors.
INAPPROPRIATE EMOTIONAL DEVELOPMENT
The clinical history of borderline clients frequently shows that they come from highly disturbed families, with a high percentage of fights and separations. In general they were children who suffered a wide variety of childhood abuse, such as:
- Physical abuse — they were victims of physical violence or were present when family members were beaten.
- Sexual abuse — they experienced incestuous relationships and/or different forms of sexual insinuations on the part of adults near to them. Kroll, (1993:55-56) says: “Our unified point of view is that episodes of childhood sexual abuse have been the most frequent cause of problems that lead to the borderline personality.”
- Emotional abuse — they suffered neglect and lack of care on the parents’ part, where an inversion of dependence was frequent and the child began to take care of the parents rather than the opposite.
Self-destructive behavior in borderline clients would be unconscious ways of perpetuating abusive parents.
As far as development phases or at what moment in the client’s life this pathology takes root, the age of 18 to 30 months, shortly after learning how to walk is often mentioned in specialized literature (Mahler,1977:82-95; Erikson,1968:107-115). Parents in this period oscillate between controlling the child so that he does not hurt himself (since he recently began to walk), or becoming slightly absent – prematurely freed from caring for a child who now would rather explore the world than passively remain in the parents’ lap.
In reality, many parents cannot stand the children’s autonomy, become resentful and threaten them with abandonment. Malher describes this period as one of separation-individualization and believes that it is crucial to the development of a separate and secure self. He observes the children of mothers who either excessively abandon or overly possess them. These children develop an intense fear of abandonment or a premature omnipotence of the type “I don’t need anybody”, for fear of being suffocated.
Erikson describes this same phase, however, in terms of polarization between search for autonomy (attempt to impose their desires), and shame and doubt (in the face of failures). The child is still very dependent on the environment and his desire for self-affirmation, intense and violent, is greater than his ability of being able to impose himself. The borderline disturbance would be the consequence of an overly authoritarian upbringing, whose strict parents would always impose their desires on the child. With time, the attempts at self-affirmation succumb to the parents’ desires and the child ends up becoming used to always submitting himself, developing a feeling of doubt about his own capabilities and shame over his failures. Little by little, he stops trying to express his wishes.
CONSTITUTIONAL FACTORS
What is found in literature only suggests the presence of constitutional or hereditary factors in this condition’s etiology. For example, we know that siblings raised in the same family react to conflicts in different ways and only a few become borderline. This shows that something specific is needed to create one type of disease and not another. However, the individual who will later develop a borderline disturbance condition is, from childhood, a hypersensitive child who asks too much from his environment; he is more vulnerable, his needs are already shown to be very intense, his threshold for frustration is less, and his reactions more exaggerated.
It is also known that anti-depressant drugs and even anti-convulsive ones have the effect of alleviating symptoms in some borderline clients, in spite of not producing changes in basic personality.
Some other studies (Stewart and Montgomery, 1987:260-266) suggest a relationship between impulsive actions and abnormalities in the serotonin metabolism. Paul Andrulois and contributors (1980:47-66) point out the prevalence of neurological disorders such as hyperactivity, attention deficit disorders, epilepsy, etc. in borderline adolescents.
Finally, the presence of borderline parents (one or both) is extremely relevant in clinical histories. However, it is impossible to determine at this moment if this signifies a biological or psychological inheritance.
SOCIOCULTURAL FACTORS
Some authors correctly point out that there are sociocultural conditions contributing to the high incidence of narcissistic and borderline disturbances nowadays. The lack of a nuclear family structure composed of a mother and father who spend part of the day taking care of their children is one of the points most often cited in this type of analysis.
The change in the role of women over the last thirty years ended up radically changing the domestic routine: the famous “dad works and mom takes care of the kids” does not exist anymore, because now ”mom is also working outside of the home”. The children go to school early or remain in the care of others and old people are treated with disdain, which contributes to one losing the sense of pertinence and history, family closeness, and reference to consistent social roles.
Other factors like technological advances, especially in the computer area, contribute to people being more and more self-sufficient and having isolated work and study routines.
We live in a “borderland” where we stimulate assertiveness (which in extreme doses borders on aggressiveness), individualism (which favors loneliness and alienation) and self-preservation (“each one for himself, God for all”).
Our society needs consistency and reliability and is extremely alienating, favoring the appearance of a gamut of pathological behaviors, such as drug addiction, eating disorders, criminal behavior, etc.
Religious sects which try to organize reality in a very simple and polarized way – ”what is right and what is wrong” – gain popularity, perhaps as a reaction to a certain nostalgia for the old days when an organized family set up rules for how to live.
Kreisman (1991) makes an interesting comparison:
We quickly moved ourselves out of the explosive ‘We Decade’ of the 60’s into the narcissistic ‘I Decade’ of the 70’s, and from there to the materialistic and fast ‘Power Decade’ of the 80’s. Following these external changes, internal changes occurred in our values: from the ideology aimed towards others, the ‘peace, love, and brotherhood’ of the 60’s, to the ‘self-awareness’ of the 70’s, and from there to the ‘self-searching materialist’ of the 80’s.”
We know that many physical diseases like stress and all the disorders it produces, such as heart attacks, hypertension, etc., are closely related to lifestyle. Why not think the same about mental diseases? They are perhaps the psychological price we pay for our modernity.
PSYCHODYNAMIC – HOW BORDERLINE WORKS
Imagine a person who because of some congenital mistake is born without skin: any touch, even the lightest one would cause intense pain and reaction. This is the borderline; what he is missing is the “emotional skin”. Searching in a simplistic way for this pathology’s formula, we might think that an overly sensitive child in contact with an invalidating and multi-abusive environment, which destroys his basic self-confidence, has a tendency to develop defensive behaviors which are going to make up the very characteristics of this disturbance.
An environment that offers little validation is one, which does not teach the child how to adequately deal with his emotions. This learning process includes not only recognizing and naming the different emotions but also learning how to externalize them, hold them in, deal with frustrations, and above all to believe in one’s own emotional responses as a valid form of interpreting the facts (basic self-confidence). What is peculiar about this learning process is that it is in large part non-verbal: children learn not only through what adults say, but especially through subtly observing how they truly are and act.
These clients’ dysfunctional families tend to deal inconsistently with emotional manifestations: sometimes they ignore; sometimes they minimize and do not confirm; and in some extreme situations, they support and shelter. It is from this inconsistent performance that some children learn to focus their energy in accomplishing something “great”. This makes them feel noticed and valued, but detours the attention needed to adequately deal with reality away from routine matters. Little by little, they become less competent, more dependent, and less responsible than the other kids.
Because of this, the borderline as adult tries to keep himself close to a caregiver at all costs. His attitude is passive towards what he must do, but he is extremely active in seeking out someone that will do it for him. This is accomplished in many ways: for example, remaining chronically sick psychologically (depression, anorexia nervosa, alcoholism), or physically (colds that do not go away, general hypochondriac complaints); presenting himself as a very naive person without any maliciousness to then set up a manipulative relationship; creating a great amount of trouble in these relationships and being the eternal victim – never receiving justice and always fighting for his rights, etc.
The people who live around the borderline, therapists and family members, have the sensation that they are going around “walking on eggs”. They often say he is never satisfied and the situations that he creates do not seem to have a way out. He has to have something to complain about, perhaps, to keep someone close to him trying to satisfy him.
Besides this, as he comes from an environment that neglects the growing child’s basic dependence needs (Cukier, 1995:65-69), the borderline remains fixated on searching for a good caregiver, the “perfect” one. He idealizes and disappoints himself easily, becoming furious when noticing other’s imperfections. He is like a child who imagines that his mother knows and can do everything, and he does not admit the opposite hypothesis.
When he grows up, the borderline ends up reproducing the invalidating characteristics from his environment: he invalidates his own emotional experiences and looks for other interpretations of reality. He is incapable of solving routine problems and has generalized difficulties about “how to live”. He sets unrealistic goals for himself, does not value small achievements, and hates himself for his failures. The “shame” reaction, characteristic of these individuals, is the natural product of an environment that shames those who show emotional vulnerability. Besides this, his suffering and emotional reactions are extreme: what would be just embarrassing becomes deeply humiliating; displeasure can become hate; a slight fault becomes shame; apprehension becomes panic or terror.
A “prisoner” of his own emotions, he needs only a small motive to provoke strong reaction such as fits of rage and violence, which confuse and frighten the people around him and himself. He creates great tragedies which he complains about with increasing rage, blaming others for the situation which he finds himself in; the greater the fit of rage, the more the borderline convinces himself and tries to convince others that they are the ones responsible for his feelings. Along with that, his emotional responses are long lasting and take a long time to return to a more appropriate emotional level. This contributes to his being highly sensitive to the next emotional stimulus.
Having his emotional development stopped in the first phases, the borderline is a child in an adult’s body. And like all children he is impulsive, does not know how to wait, cannot stand being frustrated, has difficulty in symbolizing abstract concepts (like time for example), and is always trying to get everything that he wants, at any cost. Because of difficulty in making decisions and taking on responsibility, he tends to be more successful professionally in lesser positions, preferring well structured jobs that do not demand these abilities.
In short, the borderline has tremendous difficulty dealing appropriately with his emotions, and the therapist needs to find ways: first, not to allow himself to be destroyed by emotional macro-demonstrations; second, not to destroy the precarious emotional structure that these clients show (we must remember that they do not have “emotional skin”); and finally, he needs to find creative ways of performing small “skin grafts” and give these clients some covering so they can grow and develop with dignity.
BORDERLINE CLIENT PSYCHOTHERAPY
There are two fundamental difficulties in the therapeutic treatment of borderline clients:
The first is what we could call collision of objectives, which means those goals usually accepted as valid in therapy (understanding one’s own problems, “healing oneself”, undertaking constructive changes in one’s life, etc.) are not the client’s priority aims. Initially the client does not want to heal himself; to one extent, he is proud of the symptomatology he presents, as it is witness to the atrocities that he has gone through in life. What he is looking for in the therapeutic bond is exactly this witness function: someone who sees and disagrees with the injustices that were committed against him. And he also wants (it is there where the therapeutic job becomes much more complicated) the therapist to compensate him for everything that he has gone through; he wants to be gratified for his immediate needs, be taken care of and comforted. And even more, he wants an intense and special relationship to feel important. Apparently, these client’s implicit speech is always: “I cannot get better unless you, the therapist, demonstrate that you care about me personally.”
M., 16 years old; thinking about studying psychology and not being happy with her own appearance were what brought her to therapy. In the initial interview, her parents complained about her attempts to manipulate everyone in the family to get what she wanted.
From the start, she showed herself to be an extremely insecure person, anxious to please and full of anguish. She right away established an idealized bond with the therapist, not missing any opportunity to praise her (the therapist) or recommend her best friends for treatment with her.
To investigate the purpose of these recommendations and the exaggerated idealization, an internal psychodrama was proposed (since the client refused to dramatize). After the initial warm-up T (the therapist) suggested focusing on the therapeutic relationship using role reversals, so that she could experience the two sides of the bonds.
In her own role, M stated that she was fascinated by T and wanted to get her affection in a “special way”, because this therapist, unlike the previous one, seemed to be competent and capable of understanding her. In T’s role the client was unreachable, a person who did not need anything and was very appreciative of the client and her “presents” (recommendations), however, not to the point of allowing her into the so called “special place”.
Still in the internal psychodrama, using directions so that the client could distance herself from this relationship and observe it, T asked what other relationship in her life she had felt the same way, liking somebody so much that they seemed unattainable and that no matter how much she tried to please, she could not obtain what she most wanted.
The client then remembered a scene from her childhood when she was around 4 or 5 years old in which, being out with her real father, she did everything to seem unpleasant and deny his importance: she wanted to make it clear that she loved her stepfather more, recently married to her mother and who had assumed the position of full time father. M felt very grateful to her stepfather and could not stand the idea of displeasing him. Praising him in front of her real father constituted a way of paying him homage and simultaneously getting revenge for her father’s abandoning her.
Reviewing this scene led the client to notice several of her attempts throughout her life of feeling “special”; attempts which failed systematically without exception: she had not been special to her father, who rarely visited her; she was not special to her mother, who had many priorities; and she did not even remain special to her stepfather after the birth of the couple’s new children. Her performance in therapy was just one more attempt to reach this “special” place, unattainable.
The second great difficulty treating such clients in therapy is the relationship style that they try to establish with the therapist: at the same time that they try to gratify their needs, they do not believe that this can occur. Knowing that many of these people suffer distinct forms of child abuse from their caregivers, it is easy to imagine how any bond that implies personal care will soon be filled with distrust from the past. However, firmly establishing the therapeutic bond and the sensation of being understood and accepted is the first step for the borderline client to be able to throw himself into the painful attempt of looking at his difficulties and trying to change his life.
This sensation of being accepted and understood is unknown to the borderline, who will need to check it repeatedly. His movements will be ones of advance and retreat, and the therapist also needs to advance and retreat in order to maintain this balance: an exaggerated advance or a very great retreat on the therapist’s part could put the work already done in jeopardy. The client will be constantly testing how important he is to the therapist and at the slightest sign that could be interpreted as rejection, he can attack, sabotage, or interrupt the therapy.
I., 34 years old, with a history of many previous unsuccessful therapies, starts therapy deeply depressed, crying, and without hope. Since the beginning she has been very critical of everything that T says, the way she does it or the moment she does it; in short, she is always emphasizing disagreements and making T feel cornered, having to take a lot of care not to wound her.
No attempt at clearing up these misunderstandings was very successful because the client started a confrontation, opposing her version of the facts against T’s version. It always seemed that a judge would be necessary to decide what was right.
One day T, abstracting the client’s complaints from the verbal context, began to pay attention to how much she suffered from those episodes in which she was always crying a lot and seemed to feel anguished, and that she had been treated unjustly. She decided to apologize:
– I., somehow, some things I say or do unintentionally touch an old wound of yours. I want to apologize to you for this, because there is no way that I want to induce pain or harm on you. I believe that if we are patient together, we will discover where this very sensitive point is. For now, I would like you to accept my apology, even though I don’t know what I did to hurt you.
The client became completely bewildered by T’s attitude and crying, answered that T was not to blame and that she, the client, was always starting fights in all of her relationships and that a confrontational atmosphere was common in her life. T then asked her to create a character to represent this feeling of injustice that was always attacking her, and she produced a Medieval Crusader who defended the cause of the Holy Catholic Church. I. remained in therapy for four years in individual and group sessions; she never abandoned the Crusader as a reference for these confrontational states and could, through its inter-mediation, investigate several situations of domestic violence which she had suffered in childhood. She mentioned “that day when T apologized to her” several times throughout those four years, repeatedly assuring that that was the most important moment of the therapy, without which she could not have continued.
Besides these two fundamental difficulties there are many others throughout the therapeutic process: sometimes in the middle of some simple and unimportant speech, the client rapidly escalates to extremely controversial and confrontational themes. Others, on the contrary try to please the therapist, taking on his points of view and ways of thinking, and the therapist must be careful to prevent this from happening. Many borderline clients frankly try to seduce the therapist, probably showing the way they used to obtain consideration and perhaps even some kindness in the past. Many times the therapist is taken by surprise like in guerrilla warfare: very seductive forms of relationships alternating with very aggressive ones.
Lineham (1992) and Kroll (1994) call attention to the need for validation, support, and empathy for the borderline client exactly because he lived through childhood experiences that invalidated his right to exist, have personal limits, develop individuality, and confide in his own ability to perceive and judge reality.
To validate and affirm, give permission, and gratify are therapeutic actions that many times superimpose themselves, generating confusion crucial to the therapy going well. Validation and affirmation are actions which aim at helping the client to develop an intrinsic notion of personal value, through a therapeutic relationship of acceptance which tries to illuminate the client’s positive qualities, as few as they are. This is not always easy since clients bring a huge gamut of inadequate behaviors, and it is necessary to be careful not to artificially reinforce this, which in no way would contribute to therapy. The fact that the client has survived in extremely adverse circumstances and is seeking out therapy, already represents a praiseworthy action in itself, since it takes courage to confront this journey. Real affirmation and restraint also come out of the respect that the therapist has for the client, establishing limits that he, the therapist himself, respects such as: time, space, phone calls, etc.
P., 30 years old, gets home wanting attention from his wife, who at the same time is tired and busy with the couple’s two-year-old son. His wife’s attitude is immediately interpreted as rejection and P begins to attack her, first verbally and then physically. His discontentedness and frustration increase rapidly and he cannot contain himself.
In the session, starting from the described situation and following other scene associations, we get to a scene in which he is three years old and wants to be held by his mother, who is busy cooking. She abruptly pushes him away from her and he begins to kick her out of anger. T asks the client what he as an adult would do with the child in this situation, and he answers that he would hold him before he started kicking his mother. T asks him to do it (with a cushion in the place of the child) and he hugs the cushion and cries.
In the comments, T validates both the pain of the frustrated child in the scene as well as that of the needy man arriving home; the way of dealing with his frustration and the manner of expressing his needs are discussed. One of the themes is how to contain a hurt and angry man, and the client suggests various possibilities: take a bath, go out for a walk, write a letter, etc.
Another way of affirming is to confirm the perception that the client has of his own parents and what they did to him. The therapist would be a witness to this abuse, having to help the client cry his pain and suffering away, and refocus and better organize his anger. In most cases the client turns his anger against himself, which constitutes one of the reasons for the bizarre self-destructive behavior noticed in these cases. Caution is necessary here not to excessively criticize the childhood parents because this means criticizing parts of the client himself.
M., 17 years old, 2 years in therapy, has been wanting to tell T about a subject for one month, but it is very difficult for her to approach it. Finally, she is able to tell her a “secret” which she is ashamed of and happened when she was five years old: they were at a beach house with a group of children and relatives and she allowed herself to be sexually manipulated by a teenage cousin.
Her mother accidentally discovered what had happened and became furious, harshly criticizing her in front of everybody and telling the story in a very disrespectful way to all the adults present. From this experience M concluded that she had done something very ugly, that she herself was bad and wrong, and that she should be ashamed of herself forever.
T suggests a role reversal with the frightened and guilty five-year-old girl, asking her what could have helped her to better overcome that experience. M responds that if the mother had supported her and explained what she had done wrong, along with keeping the matter to themselves, everything would have been much easier. The way her mother did it only taught her disrespect, shame, and guilt.
T agrees with her assessment, witnesses her pain and enables her to express the anger she has for her mother. The next step is to review the shame and the consequences of that sexual experience. In childhood, everything seems very serious and definitive; as adults the perception becomes relative. M contains her own little girl and gives a new meaning to the effects of this experience: nothing is totally wrecked forever!
Frequently, the borderline client tries to make the other complement him pathologically and go beyond the limits of therapy. It is always good to remember that a client’s greatest desire is to be helped to overcome the difficulties he has lived through, and it is there that the therapist must base his procedure.
M frequently requested schedule changes, giving too much importance to daily obstacles and wanting time periods which were incompatible with those of T’s. Besides this, finishing up the session at the scheduled time was difficult, since M would always bring up a very important subject right at the end. At first T tried to work around her schedule, trying to make the therapy viable.
One day after almost one and a half years of working together M, when the session finished, refused to leave the room without any apparent justification, urging T to remove her by force. After some discussion T noticed that M was overlapping the next session’s time period. T decided to let her stay in the room as long as she “needed” and to go see the next client in another empty room in her office. M remained alone in the room and after some time went away. In the following session she arrived apologizing, saying that she did not know what had provoked her into that attitude. Investigating what had happened using role reversal, M realized that she had been observing the client who came after her and felt very jealous because she was more beautiful, and “T would certainly find her more interesting”.
These associations led back to her relationship with her half brothers and parents, who “never chose her” unless she did something out of the ordinary, positive or negative. M realized how difficult it was for her to feel validated if she just behaved normally and accepted the limits that were put on her.
Permission 9 is a very complex concept, as it implies validating the right that the client has of feeling and expressing his own emotions (anger, love, selfishness) and of being respected as a human being. For example, it is normal for a client not to be able to cut himself off from people who in the past were abusive to him. The client needs to obtain this permission, therefore, in therapy.
VULNERABLE POINTS OF BORDERLINE CLIENT THERAPISTS
Borderline therapy is very delicate and the therapeutic relationship itself is firmly included. As the borderline is an eternal unloved child in search of a good caregiver, he will try to make the therapist fulfill this role. It is the therapist’s task to accept and validate the client’s feelings without entering in collusion with the part that he performs, in reality trying not to become responsible for him. The therapist needs to believe that the client has inside himself all the necessary potential for change. He must also emphasize, therapeutically, that the client recognize his emotions and confidence in his own perceptions as valid ways of interpreting reality, instead of adopting emotions and opinions from others.
The question of gratifying needs is the most crucial one in borderline therapy. As we have already said, the client’s entire performance with the therapist looks to find a place of special importance for him.
Kroll (1993), studying a wide variety of cases, mentions therapeutic and legal complications that resulted from a lack of discussion about this topic in particular. For example, legal actions alleging sexual abuse or malpractice brought by clients against therapists, threats of suicide related to certain actions that the therapist must or must not undertake, etc.
Especially questions like having or not having bodily contact with clients (hugs at very tense moments, for example), changing appointments to special days and times, permitting long phone calls at inconvenient times, etc., are small concessions that the therapist begins making almost unconsciously and which commonly evolve to the point of invalidating the therapeutic setting.
One wonders why even experienced therapists usually respond to the borderline clients’ pleas in this way. Probably due to these clients’ extreme vulnerability and a certain dose of the all-powerful savior of the world10 counter-transference that all of us have.
The excess or lack of gratification damages and may even sabotage borderline client therapy. The borderline, probably like all psychotics, has the capacity of crossing the professional line as if needing to feel the therapist’s real person. Very professional and rigid asepsis rules do not work very well with these clients, since they feel devaluated, unconfirmed, and become furious.
It is very hard for a client who has lived through these difficulties to hear the truth. This “child inside an adult’s body” does everything not to notice that his childhood has already passed him by, and that the rules and privileges of the adult world are different. Because of this, support and empathy are constantly fundamental. Without them, the borderline does not listen to the therapist’s statements about reality because he feels misunderstood and fights with the therapist.
This therapy’s difficulties are innumerable: the borderline client lives in a state of intense suffering, and many times the situations advance and become so complicated that it becomes difficult to focus on the fact which produced them. The sensation is one of building a house in the middle of a hurricane, which can seem very discouraging to the therapist.
Besides this, as the borderline deals poorly with all of his emotions, he also deals poorly with anger, being frequently subject to aggressive and explosive behavior. The risk here is that the therapist ends up “over-interpreting” the anger, without noticing what it hides – an intense vulnerability.
Finally, it is necessary to warn of the danger Lineham (1993:97) calls “blaming the victim”. In the beginning of treatment the therapist sensitizes himself to the client’s intense suffering and tries to reverse it. However, little by little when he realizes that his efforts seem useless, he can start to blame the client for causing his own degradation (he is the one who does not change and is fighting the therapy).
What is happening here is that the therapist ends up observing the behavioral consequences (the client’s suffering and the suffering that he is inflicting on the therapist) and attributing this consequence to the client’s internal and deliberate motives. In this situation it becomes very easy for the therapist to resign himself to failure, blaming the client for interrupting the treatment and relieving himself of responsibility.
THE BORDERLINE CLIENT IN PSYCHODRAMATIC PSYCHOTHERAPY
“There seems to be nothing for which human beings are less prepared and the human brain less equipped than for surprise”.
Moreno
Keeping in mind psychodrama’s relational character, it is easy to see its appropriateness for treating borderline clients in which the client-therapist relationship is the fundamental instrument.
Psychodrama, thanks to its technical resources, subtly manages to enter the client’s intrapsychic defense areas, enabling him to relate to separate parts of himself. Besides this, it is an intense therapeutic relationship that offers a chance for “live correction” of relationship forms.
It is a dialectic movement between entering the behind the scenes of psychic life where relationship wounds from the past are stored – creating armies of characterological l defense – and the return to the here and now from a validating and warm relationship which, besides being a witness to past pain, offers a new and repairing relational model.
The borderline client, used to defending himself verbally, surprises himself with psychodrama. He is not able to control or predict either the therapist’s actions or his own reactions and associations.
This represents a great advantage for the therapist, who must however be careful with the client’s timing and sensitiveness. Many times the client appears quite warmed-up, bringing up material of an intimate nature as if he were impulsively revealing all of his pain. Getting close too abruptly runs the risk of coming across a lack of prepared structure on the client’s part, who later will invariably feel harmed. Many times it is a matter of cooling the client down for him to slowly descend into the depth of his questions and act in a responsible way according to his self-exposure level.
N.L., 50 years old, two years in individual therapy, begins a therapeutic group session in which the people hardly know each other and appear careful and hesitant, being the last to introduce herself. She speaks aggressively, saying that she was not there to waste time that she had been raped as a child and still today was searching for dangerous experiences, such as having sex with anyone who appeared in front of her. The group becomes stupefied, nobody says anything, and the client becomes angry and initiates an argument.
T interferes, showing her that what she referred to as a “waste of time” was a normal way for the people to gradually get to know each other to be able to build up bonds of mutual trust, in which each one’s privacy could be respected. In the rape scene that she told about, her privacy had not been respected and the way that she presented herself to the group ended up being a type of self-rape, where she neither respected herself nor the group.
In the above-mentioned case, T just pointed out the speed and intensity that the client wanted to initiate the relationships. Other types of overly warmed-up clients demand a few technical resources to help them cool down. Carefully setting up scenes, asking for role reversals, using objects from the room, and carefully interviewing supporting characters are ways of strategically cooling down.
P, while setting up the scenes, would already start playing the roles and counter-roles speaking angrily, barely giving enough time to compose the scenery. She seemed that it was a waste of time to specify the space, as if she were always being pushed by an urgency to finish the job quickly. One day T asked her, after she had quickly described her bedroom, to switch places with the door key. She seemed completely surprised and said abruptly that she had never had a key in the door. Then T asked her to take on the role of this door without a key. All choked up, she said that the door did not protect her privacy and that through it a father came in during the night to look at her naked.
The double technique is valuable but dangerous to be used with the borderline. Caution should be shown mainly in the question of timing, as was pointed out earlier, because the client easily denies the double if it is not synchronized with his vulnerability. As a matter of fact, the best double for an infuriated client is the one which points out the sadness, the hurt, and the deception that led to the defensive response. Many times feelings of humiliation and shame are also involved.
A double that points out the manipulative character of a client’s aggressive behavior needs to be carefully introduced, and only after the affirmation of his weakened aspects.
R 30 years old, two years in bipersonal therapy and six months in group therapy. Comes to the group session angry at the other group members, who had agreed to call each other and go out during the week, but nobody called her. She tells the group:
-You really can’t trust anybody! You guys are all talk, but deep down you are as irresponsible and stupid as everybody else! I don’t know if it is worthwhile having therapy if the people are so set in their ways and don’t care about other people’s feelings. I will never make plans with you again!
Various people in the group tried to justify their absences, but R replied to them all with growing fury, not accepting excuses and invalidating any conciliatory attempts. T made a double of the group telling R how the group felt impotent since she did not accept anything they were offering her.
R became even angrier, saying that now the group was the poor one and she the villain, when in truth the situation was the reverse. Then T placed herself at her side and, imitating the same bodily position, said in a low voice:
– I would like so much to be understood, not accused . . . I feel so sad . . . I would like so much to have been with you guys during the week . . . everything got screwed up! And now . . . everything is getting even worse . . . I don’t know how to fix it . . . I am feeling more and more alone!
The client began to cry a lot after finishing the double and was able to change her attitude towards the group which, at the same time, managed finally to get closer and talk to her.
The mirroring technique is very useful for permitting a view away from the power struggles involved in the interactions, as well as the Psychodynamic produced. The therapist in this situation can formulate a synthesis of what the scene shows, accentuating parts that the client probably still does not realize. It would be like a reinterpretation, in loco, of facts that the client had interpreted differently.
L..,20 years old, is becoming an alcoholic, getting more and more involved with hard drugs. She says that she is not capable of resisting drugs when she knows that there is the possibility of getting them. However, after using them, she feels very bad and regrets allowing herself to take them.
Starting from the scene in which she gives in to drug use, L gets to a scene where she is four years old, alone in the house, feeling sad and abandoned. While she plays with a big ball all alone, she thinks that if she hurt herself, her parents would have to come home and take care of her. In continuum, she throws herself against the wall with all her might, injuring her head which begins to bleed.
Her parents are called and immediately return home to help her. Although in pain, L is happy: her parents are worried about her and together with her. It was not such a bad price that she paid!
T, leaving the positions marked off by the cushions, asks her to leave and observe the scene from outside it. T stimulates the client to observe what is happening to that little girl from her present adult role.
– Look at what is happening to that little girl. She is learning to hurt herself; attacking herself is a good way to get attention, and this is what she is going to continue doing in her life. Her capacity for self-destruction will continue growing: she will get involved in car accidents, consume great quantities of alcohol, begin to take harder and harder drugs . . .Do you think that is what she really wants? Before she started to hurt herself, what do you think that she needed? L. sadly observes the little girl, saying that she needs love and affection, but that those parents were incapable of spontaneously giving that to her. T then asks her as an adult to hold her needy little girl and see if together they would like to maintain the self-aggression and self-destruction pact, if they keep on thinking that it is a reasonable price to get love and attention.
L., holding in her arms the cushion that represents the little girl, speaks to her affectionately, saying that this was not what she wanted and that it would be necessary to find another way, but that it would take time because she did not have any idea how she could do it differently.
Mirroring is therefore a privileged place of insights for the client and therapist, but it is important that the therapist be faithful to what the client brought, not adding personal content or theories.
The technique of Supplementary Reality becomes a valuable resource to be used in borderline client therapy, since it permits him to catch a glimpse, even though in a fantasy, of the necessary solutions for the various dead end situations which are frequently proposed.
B., 27 years old, four years in individual and group therapy. Complains of professional dissatisfaction, because he always ends up having to take on greater responsibility than his partner in the firm. He feels incapable of discussing this matter with his partner without becoming internally resentful and aggressive, since his apparent attitude is one of submission and impotence.
In a scene in which he was presenting this reaction in front of his partner, T asks in what other situation from his life he had felt that same way.
Promptly, B brings up an old scene, which is already well known by T, in which after the suicide of his mother he desperately tries to please his father, even though feeling a lack of justice.
The six-year-old child, weak and helpless, does not have any alternative without anybody who could care or trust in him.
Invent the parents that you would like to have, T suggests.
B, visibly fascinated, chooses two people from the group, whom he likes a lot, to play the role of these ideal parents – caring, affectionate, and encouraging.
He spends a lot of time “enjoying” and perfecting his parents until he is satisfied.
Let’s go back to the scene with your partner except this time you will have these “good parents” behind you, who are going to cheer for you.
B looks at his partner, looks at his “parents”, who stare at him with tenderness; his posture becomes more erect and he talks calmly with his partner:
I have been very unhappy for a long time with the way things are going in the company. I think it is important that we discuss the matter in depth, because I have considered breaking up the partnership.
In the following session B tells us that the “false parental couple” seems to have injected him with an energy that is helping him to solve not only the partnership situation but also other unsolved situations in his life.
A very useful technique for working with the client’s aggressive aspects is a combination of anger concretization with the interpolation of a metaphor, which can symbolize the concretized product.
Cukier (1995:101-107) describes this character interpolation technique well. She shows how, through the relaxation of the client’s interpsychic area, experiencing reactive and defensive roles is made possible, highlighting them from the rest of the personality.
A., 43 years old, two years in bipersonal therapy, complains of debilitating jealousy of her husband and frequent crises of aggressiveness triggered by situations in which she feels insecure as a woman.
On one of these occasions, she sets up the scene of her husband getting home early in the morning. T suggests:
Show me with your body. . . without talking . . . how you are feeling.
The client lifts her arms and draws back her lips, exposing her teeth like fangs and forms her hands into claws as if she were as a beast.
Force the tension even more, T suggests. The client tenses up completely and seems like a monster twisted in rage.
T allows her to experience this bodily tension for some time, and after assertively suggests:
I want you to find a character now . . . from history . . . movies . . . any character who could feel like this.
Anything . . . the client asks.
Yes . . . the first thing that comes to your mind . . .don’t censor anything.
A tellurian woman . . . she answers firmly.
What are you like, tellurian woman? asks T curiously.
I am half woman . . . even sensual . . . and half beast . . . like a jaguar with its fangs ready to rip its prey apart.
From then on, T interviews this tellurian woman quite a bit. She tries to find out its background, when it first appeared, where its power comes from, if it even has any, etc. After this warm-up in the role, T asks the client to return to her own role, to be herself and tell her when and why she needed to create this tellurian woman inside of herself.
The client quickly brings up a scene in which, at five years old, she was taken to a psychologist’s office against her will. As soon as she got there, she began to kick, scream, and one time broke an office window. Her tellurian woman was a form of childhood defense that she had created against the impotence she felt being treated as crazy. She became “crazy” for revenge against being considered “crazy”.
In many other sessions the “Tellurian Woman” metaphor was used and even a collage was made to concretize it more. It ended up being a type of jargon between T and the client each time they wanted to refer to these aggressive defense reactions, which deep down denigrated her more than they defended her.
We believe that when a borderline client begins to understand the defensive nature of his aggressive parts, they acquire dignity and he can already stop identifying with them. He can now actively search for a more skillful way of defending himself, and this technique — the adding together of concretization with interpolation of metaphors — is extremely useful for this purpose.
Finally, we would like to comment briefly on the basic psychodramatic technique — role reversal. Experiencing the role of the other allows the client to absorb aspects of the relationship that he had not imagined. It also enables the therapist to have a more global view of the process’s psychodynamic.
Frequently, when we are investigating childhood scenes with borderline clients, we come across an “Other”, an abusive adult. It is important that the client has confirmed his abuse experience, but it is equally important that from time to time he can rescue some positive aspect from these primary relationships, without however denying the abuse suffered and the consequent emotion.
S., 28 years old, who was systematically beaten with a rod during his childhood. He tells T, when T interviews him in the mother’s role, that the mother herself was beaten during childhood with a copper wire. Her intention, when beating her son with the rod, was to give him the same education but hurting him less.
Asking questions about the abusive adult’s real intention could save, in this case, even a kind aspect from the mother, which in some way comforted the client.
CONCLUSION
Treating borderline clients presents a constant challenge for the therapist. The pain of a childhood lacking in basic care and validation saturates the possible forms of relationships for these clients, making them suspicious, demanding, scheming, and forever dissatisfied. Reaching a balance between attitudes of acceptance, support and validation on one hand, and the placing of structured limits on reality on the other, presents a difficult task for the therapist.
The seductive role of “savior”, trying to fill the client’s enormous needs, or the one of “blaming the victim”, making the client responsible for the therapy’s failure, are constant traps in the way of this task.
The creation of an “emotional skin” that can help the client to contain and organize his emotions, happens in a creative therapeutic relationship by way of small “skin grafts”, which allow us to give these clients some covering so they can grow and develop with dignity.
BIBLIOGRAPHICAL REFERENCES
- American Psychiatric Association (1995) – “Manual de Diagnóstico e Estatístico de Transtornos Mentais” – 4 ° edição. Editora Artes Médicas, Porto Alegre DSM IV pp. 617
- Cukier, R.(1995) -” Como sobrevivem emocionalmente os seres humanos?” Revista Brasileira de Psicodrama, vol.3 Fascículo II, São Paulo.
- Cukier , R.(1992) – “ Psicodrama Bipessoal – sua técnica, seu paciente e seu terapeuta “ Editora Ágora, São Paulo.
- Erikson, Erik ( 1968) – “ Identidade, Juventude e Crise”, Zahar Editores, Rio de Jáneiro.
- Falivene,L.(1995) – “Jogo: Imaginário autorizado e exteriorizado” ” in “O jogo no Psicodrama” Júlia Mota, Editora Ágora, São Paulo.
- Lineham, M. Marsha (1993).- “Cognitive Behavioral Treatment of Borderline Personality Disorder “ Guilford Press.
- Herman , J.L (1992)- “ Trauma and Recovery” Basic Books, NY,
- Kreisman, J and Strauss,H. (1989)- “I hate you don’t live me- Understanding the Borderline Personality”. Avon Books, N.Y.
- Kroll, Jerome (1993)- “ PTSD/ Borderlines in Therapy: finding the balance ” W. W. Norton and Company Inc.
- Mahler, M. (1977)- “ O Nascimento Psicológico Humano”, Zahar Editores, Rio de Janeiro.
- Miller, Alice ( 1979) – “ O drama da criança bem dotada ”. Editora Summus,1997.
- Millon, T. (1987) – “ On the genesis and prevalence of the borderline personality disorder: A social learning thesis “ , Journal of Personality Disorders 1 in Marsha Lineham (1993) em “Cognitive Behavioral Treatment of Borderline Personality Disorder “. Guilford Press.
- Paul ª Andrulois and col. (1980)- “Organic Brain Dysfunction and the Borderline Syndrome” Psychiatric Clinics of North America 4. In Kreisman ,J. ( 1991).
- Stewart ª Montgomery (1987) – “The Psychopharmacology of Borderline Disorders”. Acta of Psychiatry of Belgium 87 .in Kreisman, J. (1991)
4 Diagnosis and Statistics Manual of Mental Disturbances – 3rd edition – DSM-III Magazine – R, São Paulo, Manole, 1989 pp 366-367.
5 Does not include suicidal or self-mutilating behavior, described in item 5.
6 Kreisman introduced the term para-suicidal behavior in 1977 to mean intentional, non-fatal, self-destructive behavior (self-mutilation, taking drugs, burning, suicidal thoughts). It includes suicidal gestures and manipulations. Para-suicidal however is a better and less pejorative term than manipulator. The difficulty in treating these individuals makes one frequently blame the clients, which obviously does not help them.
9 Alves Falivene (1994) shows that in every group (family, for example) there are sociometric conditions that constitute “external authorization” for individual behavior. Each person who is exposed to this power will develop a corresponding “internal authorization”. In extremely hurt clients the internal authorization is so fragile that the demand will be a repeated dependence on the external permission. The equilibrium between an external and internal authority will be the base of a true authority. The therapist, upon permitting and validating emotions and behaviors, functions as a new external authority who looks to reinforce the client’s internal authority.
10 Miller (1979) skillfully shows how a good part of therapists come from families in which they had been asked to be the “good kids” who helped their parents.
-
EMOTIONAL SURVIVAL
For some time now, I have been coming across clinical questions, which have aroused my curiosity and resulted in this paper.
The first of these refers to the fact that after some time in therapy, we notice the existence of some nuclear scenes that seem to attract client associations like a magnet.
They appear to be matrix scenes, where something fundamental was initially structured as a defense for a traumatic situation. Through time and use, they ended up becoming part of the client’s basic identity and character.I will briefly describe four clinical cases to illustrate the point I am trying to make:
Client A – successful businessman, 34, depressed by marital problems. He complains that since the birth of his first and only child, his wife has not paid him enough attention. He suffers from bouts of physical violence that he cannot control, breaking objects at home and even hitting his wife. In one of the scenes that he frequently brings up during his associations, it is dawn, he is five years old, and he hears his father beating his mother; in another scene, he is four, his mother is cooking and he is behind her, asking to be held. His older brothers make fun of him, calling him “sissy”. (sic)
Client B – An extremely good-looking young lady, 25, who lives in almost total social isolation. She complains about depression and persecution by her colleagues, whom she considers her rivals. Professionally, she never sticks to a job, as she feels a compulsion to go out with her bosses. A little while later she is fired. She says she wants to get married and be wealthy. Among the nuclear scenes she brings up, I point out two: in the first, she is six years old and lives with her grandparents. Her mother, who is a single parent and a domestic worker, comes to visit her on Sundays. They are all having lunch together, and her mother decides to teach her good table manners, which she learned in her employers’ home. The client feels belittled in front of the people her mother admires. In the second scene, she is five or six years old and is going to ask for her grandfather’s blessing before going to bed. She knows that her grandfather would not give his blessing because he always said that he would never give his blessing to the bastard daughter of a no good mother. In this scene, the grandfather again humiliates her, repeating his bad treatment.
Client C – a 27-year-old man, in therapy for 5 years. He shows generalized difficulties in making social contacts, leading a life restricted to home and work. He has very few friends and has never had a girlfriend, even though he has fallen in love before and been interested in women. He is often overcome by anger against those who for some reason do not trust him, saying that he admires the power that Adolph Hitler had to avenge himself against those he did not like. In one of the scenes that are often repeated in his associations, he is four or five years old and his mother is fighting with him (he does not remember why). He locks himself in the bathroom and bites the plastic shower curtain in anger. When his mother catches up with him, she violently beats him on the legs with a stick until he bends over and apologizes, swearing never again to do anything that she does not like. In another scene, the client is between five and six years old, accepts a toy from a watchman who takes care of a construction site across the street from his house, and ends up being sexually abused. Only much later does he understand the fact’s significance, deeply regretting and afraid of being less of a “man” than the other boys.
Client D – a 35-year-old woman, important executive at a multinational company, reasonably good-looking who, however, complains of loneliness, an empty existence, and problems in social relationship. She usually has boyfriends for only a short time and never knows the reasons why her boyfriends break up with her; she believes men are no good. At home and at work she is seen as a troublemaker, stupid, and feels that these criticisms are extremely unfair because she “always does everything to help everyone” (sic). One of the recurring scenes in her associations is her parents’ farewell when they emigrated from Europe when she was seven years old. She wanted to cry but could not because her mother was very sensitive and would cry too. She behaved like a little “controlled” (sic) adult. In another scene, she is seven or eight years old and listens to her grandmother’s intimate secrets that her marriage is no good, insisting that all men are womanizers and unfaithful.
So, these four clients suffered various forms of child abuse: Client A used to see his father beating his mother; Client B spent her childhood hearing her mother was no good and neither was she; Client C was beaten until he would bend over from humiliation, and was also sexually abused; Client D was forced to listen to, without being able to understand, her grandmother narrate her most intimate confessions about affection and sex.
Those four people also repeat, in their own ways, the childhood drama: A beats his wife; B became a “cheap woman”; C is, in his schizoid madness, a Hitler with unlimited power who can manipulate people as he “pleases”; client D’s love life confirms her grandmother’s opinion that “no man is any good” (sic).
In adulthood, the four dominated children from the past became powerful adults who beat, fight, manipulate, and kill (symbolically) people. What happened? Why do these people actively repeat what they passively suffered in childhood? What happens in the human psyche that so strongly imprints these scenes as opposed to other memories in which the same people had been kind and gentle? Why is it so difficult for a client to change his behavior, even if he has already understood this repetition? Would we humans be like the birds, imprinting* emotional situations and running after tennis balls for the rest of our lives believing that they are our mothers?
On the other hand, when I ask these clients to dramatize their scenes and we start to research the locus, the status nascendi and the matrix (Bustos, 1994:63-77)[1] of their present problems, I always end up facing another set of facts that captivate me. These scenes take place in early childhood, most often before seven years of age.
The content of the drama that they often bring up is of a child being frustrated and/or punished for some desire or mischief; and/or a child seeing someone at home not being respected, abused by an adult who exerts and abuses the power that he has. There is an enormous imbalance of forces, and all that the child can do is passively watch the scene and submit himself to the adult’s power.
The child realizes that the adult is being unjust or abusive, feels angry but cannot do anything except submit himself. This forced submission in turn creates feelings of shame, humiliation, and inferiority that will never be forgotten, in spite of all the efforts devoted to deny, hide, and/or change them.
In these moments of tension, the child will decide something secret, a type of pact with himself, which consists basically of an agreement for vengeance and/or rescuing lost dignity. Something like: “When I grow up and have the same physical power that the adults have, I will never allow this to happen to me or to people I love”.
In short, behind the difficulties of my adult clients, I started to perceive an almost systematic existence of a child with projects to avenge and rescue lost dignity. And exactly because of the perseverance of this childhood project, it ended up creating the current difficulties in adulthood.
Like a scratched and warped record which spins incorrectly and always plays the same piece of a song, behind the current and real drama of adults there seems to be an internal dramatic[2] that repeats the childhood drama, except that frequently the roles are reversed. The one who now abuses power and imposes humiliation and shame on others is the client himself.
Thus, over the past three years I have been going after these answers. First, I began to read exhaustively all the literature available on narcissism, self-esteem, and psychology of the ego. Finally, I came across an American approach (Melody, 1989), which describes the existence of a related pathology called co-dependence[3]. I also ended up coming into contact with studies on borderline personalities and narcissistic personality disturbances.
Within modern psychodrama, we find theoretical postulations by José Fonseca (1980) on identity matrix and more recently on identity disorders (1995:22). These are added to those by Dalmiro Bustos (1994:63-77) on the concept of clusters and his emphasis on the three basic pillars of Moreno’s Philosophy of the Moment, locus, status nascendi, and matrix, which are the guideposts of my clinical understanding. As for Moreno, besides his entire body of work, it is his courage, genius, and pioneering spirit that stimulate my spontaneity and will to create. The ideas I will shortly reveal reflect how I currently understand these issues.
HOW DOES A WOUNDED CHILD APPEAR INSIDE OF US?
Human beings exert an enormous amount of power over one another, a power of life and death. From a physiological point of view, human beings reproduce the same as all mammals and are born when they leave the mother’s uterus. From a psychological point of view, however, their reproduction is totally unique and particular. Psychologically, a human being is born little by little and not always completely, depending on his personal drive and luck to have parents who know how to manage his basic needs.
By basic needs, we mean those upon which a child’s physical and psychological survival depends. There are two kinds of them:
- PHYSICAL – a human baby is born extremely fragile and in need of physical care (food, hygiene, health, warmth, physical contact, etc.), without which it would die. The focus is on What is done to the child.
- EMOTIONAL – a human being’s basic emotional need and without which he could not survive is the need for dependence, to be able to count on others. A human being is born completely unprepared, and will only be independent and with internal resources he can count on after many years (in the middle class of our urban culture, only after adolescence). Here what counts are not having these physical needs met, but how this is done.
WHAT AND HOW IS IT TO DEPEND ON OTHERS?
To depend on another person means having to subject and submit oneself to this person’s will. The one who is dependent is the fragile and impotent one in the situation, whereas the opposite is powerful and decides whether things will or will not happen and how and when they will be done. On the other hand, to have people who depend on us is also not normally a comfortable situation. It means having to sacrifice part of our time, space, comfort and independence in favor of that person.
If we ask our acquaintances and ourselves whether we as adults like having to depend on others, it is most likely that in 90% of the cases the answer will be no. Also, the memories we have of situations of dependence are mixed with feelings of shame and humiliation.
Moreno (1946:296), when describing the function of the auxiliary ego in interpersonal relationships, points out that no matter how unified the auxiliary ego is to the client, this union is never complete because of organic and psychological limitations. He says:
“A mother is an ideal auxiliary ego for the child she is expecting. She remains so even after giving birth to the baby, whom she feeds and looks after; however a greater and greater organic and psychological distance appears after the baby is born. The mother is an example of an instinctive auxiliary ego.”
We know today that nature does not give mothers exceptional patience, and that not all of them know instinctively how to offer their children a situation of ideal dependence (Badinter, 1980)[6]. Much to the contrary, what we normally find are impatient, tired mothers who try to quickly meet their children’s needs, so they can go out to work or do the things that attract their interests.
In fact, a mother’s availability for her baby will depend on extremely complex factors. For instance, her own childhood and the way she experienced her dependence on her parents; her relationship with her husband; the family’s cultural and socioeconomic situation; whether or not today’s society appreciates the mother’s role, etc.
We know through studies of infant morbid-mortality7 how many children survive beyond the first year of life, but we do not have the faintest idea of how many survive psychologically whole because we have no idea of what this means.Our clients quite often complain about parents, talking about physical violence, psychological and sexual situations, and also lack of support and information. Freud (1914:1901) first confirmed these complaints from clients, but on second thought denied them completely, attributing these abusive parents to the client’s fantasies. Other approaches believe that to blame parents actually represents a refusal on the client’s part to take on responsibility for his own future.
Only in the last few years and due to knowledge from systemic therapy have we been able to start tracing the complex web of inter-family relationships and the nature of a phenomenon that could be called psychological contamination. This means passing on from generation to generation fundamental needs in the basic dependence relationships that end up pervading the individual’s entire human relationship capacity.
WHAT EXACTLY DOES THE BASIC DEPENDENCE NEED OF HUMAN BEINGS MEAN?
To answer this question, I must first quickly describe a child’s four natural characteristics that make him an authentic human being and are very well summarized by Bradshaw (1988).
- THE CHILD IS VALORIZED – a child is not born with self-esteem and does not have any notion of his personal value. He will absorb this value from the outside in, according to the esteem and dedication that his parents have for him. Early in life this may mean a special touch or look (Kohut, 1977) 8, constant and predictable presence, meeting physical needs correctly. Through his development, devoting value to the other will progressively be transformed into more complex attitudes and which demand great maturity from the parents, such as allowing a child to try his growing independence without threatening him with withdrawal of love.
Margareth Mahler (1977), observing child development step by step over many years, describes mothers that cannot bear their babies’ gradual detachment. They de-personify them, hindering their hesitant search toward independence instead of allowing and promoting gradual separation. Other mothers with symbiotic characteristics will first closely hold on to their babies only to then push them prematurely to “autonomy”.
An extremely powerful way of pressuring a child into doing what parents want is to tell them “If you do not do this, mommy and daddy won’t love you any more!” Another common way of playing with this power of attributing value to a child is to compare him to other children, making him feel inferior or superior to someone else. To threaten a child with no longer having the love of adults who are meaningful to him is tantamount to removing this child’s value. In other words, it consists of saying to him that he has no inner value but only relative value that is dependent on what he does or how he does it.
I think that one of the most difficult tasks in educating children is to establish limits, without however blackmailing them by removing their intrinsic value. Most parents were brought up this way by their own fathers and mothers and consider this form of communication with the child to be natural and inoffensive. If we think of an adolescent, frequently threatened with having his favorite pastime taken away from him if he does not get good marks at school, we can see how an old abstract value is over time turned into concrete objects, material goods, and money that will be given or denied, according to his behavior.
Whenever a child feels that he has no value to his parents, he feels ashamed and inferior because of this. The “I” loves and respects itself when it realizes it is loved and respected. On the other hand, the “I” hates itself when it realizes it is being rejected or left aside. Many years of education under this system of manipulating the other through giving and removing value end up by creating adults who, like Client B, survive with a sense of faulty self-value. They are people that either underestimate or overestimate themselves, becoming either excessively dependent on the other, without the autonomy of adult life, or excessively independent of the other (the kind that does not need anyone).
- A CHILD IS VULNERABLE, SUSCEPTIBLE – he does not have a developed defense system (boundaries) and depends on his parents to protect him. This lack of limits between the “I” and the “Other” makes children naturally egocentric and involved in everything surrounding them, explaining the world based on themselves. For instance: “if my parents fight, it is my fault; if they are not with me, it must be because I am bad; if they work too much and are not with me, it is because I am worth less to them than their work.” Parents have the arduous and double task of recognizing and respecting the right that children have to be owners of their own bodies, thoughts, feelings and behavior and at the same time guiding them toward a more realistic and functional perception of the world, limiting their egocentrism.
Gradual frustration of some of a child’s needs makes him realize that the other is not his intrinsic part. On the other hand, whenever a child is frustrated he reacts with irritation, stubbornness and unpleasantness. This is normal and parents must accept these aggressive impulses without letting themselves be personally destroyed by them. Expressing emotion is one of the body’s physical needs in its quest for a homeostasis that has been lost. If emotion is not expressed, it reflects back, returning to the child’s “I”. In this way anger, for example, that cannot be expressed ends up returning to the “I” itself, creating self-destructive symptoms and attitudes.
Some parents cannot tolerate children’s impulses and emotions. In fact, when emotions are very strong, adults are afraid of losing control of the child, and try to restrict him. No one can put up with an enraged child or even with an excessively happy one. They make too much noise, become overexcited and disturb us. Many parents go too far in punishing (Client C) or threatening not to love anymore, as was seen before.
We frequently see clients who from very early on stop upsetting their parents and start pleasing them, trying not to make them too irritable or depressed (Client D). There is an inversion of dependence: the child acquires the power of defining a situation and learns that his parents’ mood depends on his and not vice-versa. These are “the very nice” children who help their parents and use their sensitiveness and empathy to serve others and, according to Alice Miller (1979), those who have a good chance to become psychotherapists some day.
The parents’ independence, together with the fact that they also have well-established limits, helps a child to separate himself from them and to have a suitable internal representation of himself and others. When this does not occur, there possibly survives an adult who either does not know how to protect himself adequately in relationships or who cannot contain himself from being offensive to others (Client A). It is still possible to think of the vacillating type who at times is extremely non-vulnerable, while at others shows extreme vulnerability.
- A CHILD IS IMMATURE, IMPERFECT – he lacks coordination, drops things, breaks objects, falls, gets dirty, makes noise, puts his finger up his nose, fights in the car disturbing parents who are driving, asks to go to the bathroom at the most awkward times, etc. In short, children act as children because they lack motor coordination, knowledge of their limitations, and do not know how to act when faced with difficulties, etc.
In many dysfunctional families where adults consider themselves gods who manage perfection (they never make a mistake and if they do they will never admit it or apologize), children are punished severely and are ashamed of making normal mistakes. Children are expected to be more mature than they are, as if they had been born with a manual of information on life (Client A).
A client of mine can recall hours and hours of fear spent inside a dark bedroom, but cannot recall what she did wrong; therefore, whatever her mother wanted to teach her through punishment did not work. Through fear, shame, feeling of inferiority and helplessness, the only learning that is internalized is that we, as human beings, are worth nothing (Clients A, B, and C).
Much information is necessary for a child to understand how life is. He will learn by trial and error and/or through what adults teach, but above all, through how adults act. We know today that children brought up by overly intolerant parents usually conform to the expectations, and later become perfectionist and controlling adults. They can also become deeply insecure adults who suffer too much when making a mistake and fear evaluations; or they can rebel, refusing to cooperate and even doing the contrary of what is asked of them. These are the rebellious bad children who are a problem at home.
I usually tell my clients jokingly: – “Do what you want to do, even if your mother agrees!”, referring to this mechanism of “going against”, because what I find is that many adults do not even follow the rules they make for themselves, being incapable of any discipline.
Another inadequate way of dealing with children’s imperfections is by ignoring them, causing children to end up never learning that their behavior bothers and disturbs other people. Thus, we also raise people who will be seen as nuisances and bores by society, simply because they are not aware that their behavior is abusive and disturbs others.
Finally, I think that one of the most valuable learning processes children can have is to be shown that from time to time everyone, including their parents, make mistakes and that almost always mistakes can be corrected or at least excused.
A CHILD HAS A CONCRETE AND RADICAL WAY OF THINKING – a child does not discriminate nuances among the qualities of people and objects. Their concrete thoughts make them think in a polarized and extreme way: it is either good or bad, all or nothing, now or never, etc. Gestalt therapists (Perls, 1973:46-48) described yet another peculiarity of the infant mind: the one of assimilating introjects, whole pieces of ideas, as if they swallowed food whole without chewing it. Piaget (1926:54-74), in turn, shows us that only from 8 years of age children are able to understand separate experiences and assimilate differences. Very young children believe that they are what others say they are and that is why they are really bothered when made fun of.
So, faced with these four child characteristics: valuation, vulnerability, imperfection, and radical thinking we can infer what basic dependence needs of a human being means. It means to be able to count on parents who: make him feel precious, important and provide for his needs while still not independent; devote time and attention to help him define his own limitations and obtain information needed to deal with reality and his own needs; allow a child to express his aggressive and hostile impulses without destroying them or the child’s self-esteem, while at the same time allowing aggressive and hostile reactions to be expressed, respecting an intrinsic asymmetrical bond; allow a child to be a child to then grow up and become independent; be coherent, consistent, predictable people who teach and act in the same way; be fallible beings who admit their mistakes and apologize.
It is quite possible that when reading such a long list, the reader may consider me a demanding person, or that these ideal parents are everything but human and that one fourth of the characteristics described are already sufficient for a child to grow up reasonably normal. However, I have noticed that for each deduction given to parents, one point is added to an enormous list of child abuse.
Children subjected to any kind of abuse or who have these basic dependence needs neglected only grow physically and socially. They somehow continue emotionally humiliated, orphans, and harmfully ashamed claiming what they never had, trying at any cost to repair their self-esteem, dignity, and hurt narcissism.
CHILD ABUSE (IS IT AN EXAGGERATION TO CALL SUCH ROUTINE OCCURRENCES ABUSE?)
Studies (Kreisman, 1989; Bradshaw, 1988; 1990) on narcissistic borderline personalities and co-dependence widen the concept of child abuse, whereas in the past it was almost limited to extreme events, such as sexual abuse. Today, we consider that parents are abusing a child whenever they do not respect the hierarchy of the parent-child relationship, like when they do not protect the child or help him develop.
The parent-child bond pre-supposes a hierarchy whereby two adults decide to have a child who they will be responsible for until the child grows up. There is a legislation that regulates this relationship, which is currently being reviewed in the United States. I briefly list below some forms of child abuse:
SEXUAL ABUSE
It is the sort of abuse that is most shameful, more frequent than is imagined, and involves the whole family. It involves not only the fact that one or both parents oblige the child to have physical sexual relations with them, but also subtle forms of abuse, such as:
- SEXUAL INTIMIDATION – creating situations whereby a child sees or hears what he does not want to, what he cannot understand, or what makes him ashamed. It is the case when children who, due to parents’ carelessness, overhear or see their sexual intercourse, or even the case of adult voyeurs and/or exhibitionists who observe their children sexually and/or undress in a sexual way for their children to admire. Pia Mellody (1989) believes that sexual abuse occurs whenever a parent has a more important relationship with one of his children than he has with his spouse. She refers to the fact that children need parents, not husbands, wives or admirers; many adults make it clear that they admire their children’s bodies, that they would love to be younger so they could date them, or that they are more beautiful, smarter and able than their spouses.
- PHYSICAL CARE – for example the use of enemas or bathing older kids may be a form of disguised sexual abuse. I had a client who dried her daughter’s vagina until she was 10 to prevent the girl from getting a rash, and only stopped this after undergoing therapy.
- LACK OF SEXUAL INFORMATION SUITABLE TO AGE – for instance, not telling a girl she will menstruate, telling children that masturbation causes physical lesions, etc. Children, mainly the very young, will not always know when adults have a sexual intention. However, they end up invariably finding out, being ashamed and hurting their self-esteem. Because they do not know sexual phenomena and think radically, they imagine terrible consequences for their future and feel they are doomed to a tragic end from then onwards.
PHYSICAL ABUSE
Any kind of physical punishment – beating, spanking, pulling hair, locking in dark rooms, etc. – administered to a child or to someone else in the family while the child watches. Kreisman (1989) shows that parents who beat their children were beaten when they were children (Clients A and C).
EMOTIONAL ABUSE
Results from a confusion of boundaries within a family and from a reversal in the natural order: the children look after their parents and not the other way round. This is not only the case of children of alcoholics, seriously depressed people, etc., but it occurs in most families known as “normal”. One or more children in the family are especially encouraged to be assistants to their mother or father, many times because this adult who is asking for help is fragile and cannot defend himself against some abusive situation inside the family.
The child takes on this special role not because he really wants to but to help his parents whom he depends on, and/or ensure their love, which may be lost if they are upset. In a word, he does this to avoid loneliness and being abandoned. Paradoxically, this efficient adult-child ends up having within himself an abandoned and hurt child. As he looked after his parents so well, his own childhood needs were neither met nor respected (Client C). Another form of emotional abuse is to disrespect a child’s will and impose that of his parents. For instance, to make a child eat what he does not want to, put on clothes he hates, etc.
In conclusion, a child that does not have his needs of dependence met and respected suffers serious damage to his basic identity. He goes on disbelieving in his own needs, judging them to be illegitimate, and seeing his own desires as shameful. His infant egocentrism, added to the fact that he needs to maintain the ideals of the adults on whom he depends to survive, makes him frequently blame himself for his parents attitudes, such as: “It is me who is bad! I was bad! I am stupid! I have some serious fault, etc.”. This will, with time, become a trait of the individual’s identity.
As abuse is a secret family topic, the child judges that he is the only one in the world living that situation, being therefore of less worth than other kids. In these circumstances, the child also feels completely abandoned, orphaned and lonely because at the time that abuse or neglect occurs, there is no one to defend him. He concludes then that there will never be someone on whom he can count, because if his own parents were not reliable, who else will be?
HOW DO WE SURVIVE THEN?
In all forms of abuse, adults either exert their power over the child, acting violently against him, or waiving themselves of the responsibility of looking after and protecting him.
Freud (1905:2508-2541) was the one who first identified automatic processes used by the ego for self-preservation whenever it suffers a severe shock. However it was Anna Freud (1973) in her “Ego and Self Defense Mechanisms” who definitively introduced the question of psyche defenses to our present clinical thinking. These defenses are ways that human nature has of protecting the child’s psyche from extremely intolerable situations. This until he has better defined ego-like boundaries and knows how to separate what is his from what belongs to the other. Some of these mechanisms are as follows: denial, repression, dissociation, depersonalization, identification with the aggressor, conversion, etc.
Indeed, a child’s violated “I” does not choose one or the other of these mechanisms to defend itself. It uses many of them alternately or at the same time to form a defense system that is the most effective possible, which Winnicott (1982) brilliantly defined as “False Self System.”
FALSE SELF – OUR HIGHLY SUCCESSFUL ADULT
In a desperate attempt to try and hide from himself the reality of abandonment and helplessness that he is experiencing, a child denies or substitutes his own emotions. He creates an alternative way of being that he considers to be better appreciated by those with whom he lives and which does not have those shameful and faulty characteristics of before. This superior being rejects the true being, often in a just as cruel or even crueler way than the child’s parents. This includes the false self system which has the following characteristics.
It is always super human or sub human, perfectionist or stupid, victim, hero of the family or scapegoat, etc. This is because the emotions that the defenses will fulfill are human emotions. Without these a person becomes something unreal, like a character in a book, for instance. The roles played are as a rule pathological complements that the family requires. There are always contrasting criteria involved, criteria that follow the child’s radical and absolutist line of thinking.
Shame and lack of protection in childhood are the basic motivations for creating any of these polarities.
As soon as the false self is structured, the real self is buried and forgotten. With time the person loses the awareness of whom he really was, as well as the memory that he had created a character for himself.
The false self-function is two-sided: while it protects an abused and neglected child, it also tries to satisfy some of those neglected needs that the child himself denied. For instance, a child may attract attention by hurting himself, by getting sick, by refusing to eat or by being the best student in the classroom.
The repressed and denied parts of the ego are projected in relationships and constitute the basis for much hate and prejudice. They can also be seen as a split personality or multiple personalities (this happens with people who suffered physical and sexual violence). It creates a feeling of unreality and chronic depression for the loss of a part of oneself.
The false self is also followed by a system of constant self-observation and vigilance because we must make sure the rejected parts do not surface and make us feel ashamed or inferior. We are dealing with tortuous self-conscience that has a paralyzing internal effect.
MULTIGENERATIONAL ASPECT – PSYCHOLOGICAL CONTAGION
Parents frequently justify their attitudes to children saying that they are doing their best and believe this to be the best way to bring them up. In fact, I do not think that parents are lying; maybe some are but not all.
Indeed, we know today that the interpretation of how to raise a child depends less on rules that psychologists or educators establish as healthy and desirable, and more on the parents’ emotional structure and on how they were raised.
This is the phenomenon that I called “Psychological Contagion”, and Freud “Compulsion to Repetition” (1905:2508-2541). It is a complex, unconscious process in which, even as adults, we try to satisfy our infant needs and to rescue our wounded dignity.
Our children and their infant attitudes are seen by our wounded internal children as torturers who submit and force us to do things we do not want to. For this reason, we punish them. While children we were only capable of defending ourselves using our infant defense tactics9. These are the tactics which, though inefficient against the adults who abused us, we repeat against our children, perpetuating these abusive characteristics10 from generation to generation and within the family.
In fact abusive, authoritarian, and unconfirmed behaviors occur in all contexts of our lives. They are not only multigenerational but also intergenerational. Moreno (1992, p.225) uses the concept of sociometric proletariat to talk about isolated, neglected, and rejected groups whose feelings are nor reciprocated. We humans are specialists in the creation of these “sociometric proletariats”; because of this for example we are so afraid of presenting our ideas at conferences.
This is the “broken record” that repeats the same part of the song. Someone has to gently remove the needle from the scratched area and show the client that this damage could be repaired, mended or covered, but it will not stop existing. On the other hand, the future is full of records that can still be played if the needle is removed before it gets damaged.
HOW CAN PSYCHODRAMA HELP THESE CHILDREN BURIED INSIDE OF US?
In my life, psychodrama has meant the best technical assistance for mending “scratched records” that I have ever found.
I believe that human psyche is structured around a narcissistic economy; from the day we are born until probably the day we die, we try to determine who we are and what “our value” is to others and ourselves. Over time we may or may not modify our value criteria, but we will always be people who search for value.
For me, this is the intangible part of the “I”, which is behind the role. And I am not as sure as Moreno (1992:185) 11 about which of the two parts comes out first and creates the other. I think that this search for intrinsic value is part of human nature, but I will talk about this at another time.
The drama of the wounded child that many of us maintain inside ourselves relates to a time in our lives when our narcissism was weakened. Our psyche then went into action in all its spontaneity to repair the damage done. We created a specific antibiotic for the problem that assaulted us and kept it up like a precious stone, thinking about using it each time that another threat to our self-esteem appeared in our way.
However, the antibiotic’s expiration date passed and somebody needs to convince our hurt child that his medicine is old and that it must be thrown away. In fact he already knows this – that is why he turned to therapy. However he doesn’t know how to use another medicine, so he sticks to the old one. Talking about it is not enough.
I think that there is nothing more alluring for a child, even a sick and depressed one, than giving him a new toy or suggesting a different game. I know this because I worked12 in a children’s ward for terminal diseases for a short time and they would play with me. The game’s “as if “ decentralizes our basic identity and for some time we can forget who we are, our pain, the illnesses we suffer from, and how we can prevent them from reoccurring.
Furthermore I can be whoever I choose in a game, from a gentle princess to an angry Hitler. Whoever I choose to be, the fact is that for a few seconds, I stop being myself.
As I see it, one of the strongest therapeutic forces of Psychodrama is exactly in proposing techniques, by means of an elaborate warm-up, that will free a person from his basic identity and enable him to see beyond what his own eyes could not see. In the role of another person, I can see and speak of things that in my own “I” I could not. Moreover, the “as if” concretizes situations, affections and personalities that otherwise would be mere abstract ideas, without sufficient embodiment to involve anyone. For instance, through Psychodrama we can characterize and concretize our child within, talk to it, exchange roles, etc.
Through open scene dramatization or internal psychodrama, using all classical techniques and following the transferential chain of client associations (Perazzo, 1987) 13, I find it quite easy to bring these childhood dramatics to the surface. I have learned through experience that therapy as it is practiced can only start when a client repeatedly identifies this child and starts to take it seriously. He will no longer go on blaming others for his problems and will start to assume responsibility for his shortcomings.
On stage, the drama that starts to be played is not so much between a client and his social atom but between himself and his own parts and fragmented characters, each one a holder of a part of his own infant defense system.
My greatest problem at present is to help clients make agreements with their hurt child within, because like all children they are stubborn, obstinate, and do not negotiate when not getting what they want. Except that no one can give them exactly what they want – the past does not return. An adult client must, at all costs and like a tolerant and persistent parent, help his infant side to deal with frustration, to make agreements, rationalize in less extreme ways and express his dissatisfaction in a less angry way. This is what I understand by re-matrix and what Moreno (1992:153) means when he defines spontaneity as the “driving force of an individual towards a suitable response to a new situation, or a new response to an already known situation”.
I invent games, adult-child confrontation situations, ask clients to write letters to their child within, encourage role playing and metaphor creation, and assimilate techniques from other approaches. In group therapies I propose meetings with all the clients’ hurt children . . . in short, I love seeking new ways to help people in this task.
However what I really know to be effective is to offer, through the client-therapist relationship, respect and acceptance, consistence and commitment, along with the therapist’s emotional capability toward the client’s real drama. These are magic potions and Moreno was a master of them. In this existential meeting I am 100% Morenian.
When she was in Brazil in 1993, Zerca Moreno (Cukier, 1994) began her speech saying that within everybody lives a hurt little child and considered the urgent creation of schools for parents a preventative and public health matter.
I was exhilarated when I heard her and thought to myself: Would Moreno agree with this, if he were alive?
I will never know the answer but can find out what you, who represent the modern psychodramatic movement, think. I am waiting for your answers.
BIBLIOGRAPHICAL REFERENCES
- Badinter, Elizabeth, Um Amor Conquistado – O mito do Amor Materno, Editora Nova Fronteira, 1980.
- Bradshaw, John, Healing the Shame that Binds You – Health Communications, Inc., Florida, 1988.
- Bradshaw, John, Homecoming, Bantan Book, N.Y. 1992.
- Bustos, Dalmiro M, Asas e raízes – Locus, Matriz, Status Nascendi e o Conceito de Clusters in Leituras 2, Companhia do Teatro Espontâneo, 1994, São Paulo.
- Cukier, R., “E a Zerca veio . . .” in Revista Brasileira de Psicodrama, Issue II, 1994
- Erikson, Eric, Infância e Sociedade, Zahar Editores, R.J. 1976
- Fonseca, José F., Psicodrama da Loucura, 3a. edição, São Paulo, Ágora, 1980
- Fonseca, José F., Diagnóstico da Personalidade e Distúrbios de Identidade – unpublished article.
- Freud, S, História do Movimento Psicanalítico in Obras Completas, Madrid, Biblioteca Nueva, 1973
- Freud, S, Mais Além do princípio do Prazer in Obras Completas, Madrid, Biblioteca Nueva, 1973
- Freud, S, Os Instintos e seus Destinos in Obras Completas, Madrid, Biblioteca Nueva, 1973
- Freud,A, O Ego e seus mecanismos de defesa, Editora Civilização Brasileira, R.J., 9a. edição, 1990.
- Kreisman, J Jerold and Strauss, H., I Hate you – don’t leave me – Understanding the Borderline Personality, Avon Books, N.Y., 1989.
- Kohut, H. Self e Narcisismo, Zahar Editores, RJ, 1984.
- Mahler, Margareth – O nascimento Psicológico humano- Zahar Editores, RJ, 1975.
- Mellody, Pia, Facing Codependence, Harper & Row, Publishers, San Francisco, 1989
- Miller, Alice, O Drama da Criança Bem Dotada – Summus Editorial, 2a. edição, 1986
- Moreno, J.L.-Psychodrama – Editora Cultrix, São Paulo, 1975
- Moreno, J.L., Quem sobreviverá: Fundamentos da Sociometria, Psicoterapia de Grupo e Sociodrama, Dimensão Editora, Goiânia, 1992
- Moreno, J.L, Fundamentos do Psicodrama, Summus Editorial, 1983, São Paulo.
- Perls, Fritz, A Abordagem Guestáltica e Testemunha Ocular da Terapia, Editora Guanabara, segunda R.J.
- Perazzo, S., Percurso Transferencial e Reparação, Revista Temas, ano XVII, no. 32-33, 1987
- Piaget, Jean, A Representação do Mundo na Criança – Editora Record Cultural, R.J. pp 54-74 (The first edition in French dated 1926).
- Stettbacher, Konrad J., Making Sense of Suffering, Penguin Books, New York, 1991
- Winnicott, D.W., Ambiente e os processos de maturação”, Editora Artes Médicas, Porto Alegre, 1982
- Symington, Neville, Narcissism, A New Theory, Karnac Books, London, 1993
- * Konrad Lorenz, 1973 Nobel Prize winner, conducted an experiment with geese, discovering that these animals’ first vital experiences create patterns of behavior that last for the rest of their lives.
- [1] Dalmiro M. Bustos is an Argentinean psychodramatist, director of the J.L. Moreno Psychodrama Institute in São Paulo, Fortaleza, and Buenos Aires. (See also the footnote on page 73 concerning the Morenian concepts of : locus, status nascendi, and matrix).
- [2] I used the expression “internal dramatic” to differentiate the drama that occurs intrapsychically between the client and his wounded child within from his adult life drama and from the real relationship as he lives them today.
- [3] Co-dependence: the name was coined to describe the dynamic of families of alcoholics in which the families themselves became dependent on the illness. Over time, the term became more wide-ranging and refers to problems of “normal” families who, however, do not help their members to be autonomous and independent, maintaining a permanent mutual control.
- [4] “I” is used here in the most common meaning of the word. I purposely did not use either the term “Ego” nor “Self”, so as not to enter the psychoanalytical definitions and academic discussions about this theme. “I” is the way that people normally refer to themselves and is the name of the central axis of an individual’s identity.
- [5] Erik Erikson defines identity as an interpersonal process. He says: ” The meaning of the ego identity is the confidence to internally have one single thing, a continuity . . . and this is achieved through the predictability and continuity of what I mean to the other.”
- [6] Elizabeth Badinter, in her book ” L’Amour en Plus”, shows how a mother’s love for her baby is influenced by the cultural value of the roles of mother and child. In the 18th century, court parties and public executions infatuated French society, and children were given absolutely no value. Very few women breastfed and cared for their children personally, despite the papers at the time publishing high infant mortality rates among children brought up by their breastfeeding servants (25%). Badinter is radical when she says that handing over a child to a servant for breastfeeding is a form of disguised infanticide.
- 7 According to the C.E.A.D.E. Foundation, 1992 for every 1,000 children, 26 die before reaching one year of life
- 8 The shine of a mother’s eye, according to Kohut
- 9 What I call infant defense tactics are all of those described by Freud and Anna Freud, besides Winnicott’s False Self System, seen through the eyes of a child, with the infant characteristics that I described above.
- 10 In fact abusive, authoritarian, and unconfirmed behaviors occur in all contexts of our lives. They are not only multigenerational but also intergenerational. Moreno (1992, p.225) uses the concept of sociometric proletariat to talk about isolated, neglected, and rejected groups whose feelings are nor reciprocated. We humans are specialists in the creation of these “sociometric proletariats”; because of this for example we are so afraid of presenting our ideas at conferences.
- 12 The Children’s Institute at the Hospital das Clinicas in São Paulo, in the children’s ward on the 4th floor.
-
THE PSYCHODRAMA OF MANKIND. IS IT REALLY UTOPIAN?Moreno always dreamt with the universal utilization of psychodramatic and sociodramatic techniques to help large communities in their social problems. The author discusses the urgent need to do so, in order to help many of the ethnic and political conflicts that emerge all over the world. The offended pride of a group will look for revenge during many generations.” Group Narcissism”; “ group mourning and reparation” are some of the concepts discussed in this article.
“A truly therapeutic procedure cannot have less an objective than the whole of mankind…
I predict sociometry and psychodrama will have an important place in the history of sociology as it will be written in the year 2000…
We assumed — naively perhaps — that if a war can spread to encircle the globe, it should be equally possible to prepare and propagate a world sociometry. But this vision did not arise wholly out of thin air. Once we had successfully treated an entire community by sociometric methods, it seemed to us at least theoretically possible to treat an infinitely large number of such communities by the same methods — all the communities in fact, of which human society consists…
The sociometric experiment will end in becoming totalistic not only in expansion and extension but also in intensity, thus marking the beginning of a political sociometry.”
(Moreno, 1978)
Moreno’s pretension to treat the whole of mankind by psychodrama has always seemed exaggerated and improbable to me — utopian dreams of a man who, besides having sought more regard and recognition than he had in life, had also made predictions for the distant year 2000 which he would never witness.
Having said that, I have just returned from the 13th International Congress on Group Psychotherapies held in London. This is August 1998 and we are coming very close to the year 2000. I came back thinking differently. I wanted to review these words of Moreno’s, so I read them carefully. I heard things at this congress that repeatedly reminded me of Moreno, and I am writing this paper so I can share my recent findings with you.
I was particularly impressed by the core theme of the keynotes at this congress. The lecturers, all of them professionals of worldwide renown for their scientific works, belonged to an inter-area of interest blending at one time history, sociology, anthropology, politics, and psychology. Their main concern was to be able to understand and contain the escalation of the so-called political and ethnic wars.
I will summarize some of their ideas specially some concerns of Vamik Volkan (1997), a Turkish psychiatrist whose book ¾ Blood Lines, from ethnic pride to ethnic terrorism ¾ unfortunately has not yet been translated into Portuguese.
Volkan points out that although the so-called Major Armed Conflicts [1] have reached a plateau since 1986 – around 30 conflicts in 25 localities ¾ minor conflicts , commonly known as Ethnic Terrorism [2] have undergone a startling growth ( estimation of The Institute for International Peace Research at Stockholm )
After World War II , as adopted by the UN , the term “ethnic background” ( “ethno” comes from the Greek word ethnos meaning tribe, company, people) has been used as a substitute for the term “race”, due to the connotations of biological inferiority and superiority which the Nazis lent the term race.
But new words have not changed old problems. National civility, which used to allow people from different cultures in the same nation [3] to live together in peace, has been defeated by ethnic hatred, and millions of people have died since then in “confrontations among neighbors”.
In Yugoslavia, for instance, it is estimated that 65,000 people have died on account of ethnic conflicts; in Bosnia-Herzegovina, 55,000 have died; in Croatia, about 10,000; and in Rwanda, deaths have reached one million already. And how many more people may be dying in conflicts in Afghanistan, Algeria, Angola, Azerbaijan, Bangladesh, Burundi, Cambodia, Colombia, Georgia, Guatemala, India, Indonesia, Iran, Iraq, Israel, Liberia, old Burma, Peru, the Philippines, Somalia, Sri-Lanka, Sudan, Turkey, England, and Zaire?
Our attention is turned to the barbarism of these conflicts as human rights are completely ignored and genocide is their frequent goal, and not even the ethic codes of traditional wars are adopted. We no longer talk about the “extermination of a people”. Nowadays “ethnic cleansing” is the word of command and not a single soul belonging to a different ethnic group should live – not even those who still recall the lands and homes they used to possess.
Décio de Freitas (1998) shows us that many of those who fight and kill one another may be ethnically similar in history, in blood, in language, and even in religion. Intolerance focuses not on macroscopic differences, but on subtle alliances. There is loyalty to a small ethnic group and not to the greater nation. There is a clamor for revenge on account of past resentment, a trans generational effort at any cost, to restore the dignity of a people.
You must be wondering what Moreno has to do with that. Well, the old dream of treating the whole of mankind is modern in Europe right now. The failure of the traditional international diplomacy has generated a growing demand for a change in the concept of diplomatic work which now includes the psychological dimension of events and not only their social and economic aspects.
Volkan mentioned Donald Horowitz, a political scientist, who advocates the idea that the amount of passion expressed in these ethnic conflicts calls for an explanation that takes emotions into consideration. Complex questions, briefly described below, connected to the identity of large groups, the concept of ethnicity, how a large group elaborate cultural losses, etc., are now being discussed.
THE IDENTITY OF LARGE GROUPS
Volkan explains that human beings have always lived in emotionally linked groups, such as clans or tribes. “Ethnic Group” is the contemporary term for this phenomenon, defining a number of people with something in common: their place of origin, their ancestors, their traditions, their religious beliefs, and their language. Besides these characteristics, people from the same ethnic background also share a myth of inauguration, a kind of grandiose history about the origin of their group that includes a concept of generational biogenetic continuity and lends the group some special and unique characteristics, which make it different from all the others.
The perception of one’s own tribe or group as being human and superior to the others, which are seen as sub-human, is a universal phenomenon that intrigues scientists. It seems that in the beginning, neighboring tribes used to compete for survival items such as food and water. With time, and as soon as their survival was assured, other superfluous items became targets of competition. However, once these items could boost the self-esteem of whoever possessed them, they became symbols of power. These symbols, in turn, gained particular colors, a particular flag, a song, and other cultural indicators of the shared identity and of the history myth of that particular group.
Volkan exemplifies this point describing that the ancient Chinese people used to call themselves persons and other races, Kuei, which means hunting spirits. The American Apaches called themselves indeh (persons) and others, indah (enemies). The word barbarian means foreigner in English.
Ethnicity is an aspect of personal identity; it is a social, not biological identity, and it goes beyond genetic considerations. Its major peculiarity is that it is felt only when a group interacts with another, as if it were a force that only manifests itself through interacting with a different group[4]. A certain degree of ethnocentrism is common and healthy in all groups, but it may dangerously break into a type of racism.
THE PERSONALITY AND THE PSYCHODYNAMICS OF ETHNIC GROUPS
Very little is known so far about how large groups function. Freud (1920) has made some attempts to study group phenomena. Before him, other authors, namely the French sociologist Gustavo Le Bonn (Freud, 1920) and American Mac Dougall (Freud, 1920) had tried to provide some explanations on the matter. The latter found that whenever an individual takes part in a group, he/she will loses his/her habitual identity and experiences an increase in his/her ability to become emotional and supple as well as a decrease in intellectual and cognitive abilities.
Freud attributed these phenomena to the libido, which he credited with creating and maintaining love ties in a group. To him, the group mind was structured in a manner similar to that of family models; love among group members and their ability to influence one another would be proportional to the love and respect achieved by the leader of the family. As to hostilities among members, those were attributed to poorly resolved oedipal questions.
Volkan views this explanation as incomplete, clarifying little of the question of aggressiveness in human relations or of why a sense of group identity sometimes leads to brutal acts of violence.
According to Volkan, Freud himself was cautious in applying his findings in individual psychology to group psychology. In 1932, Albert Einstein, in an article entitled “Why war?”, asked Freud whether there was any way whatsoever of preventing wars from happening. Freud was pessimistic in saying that there was no way to eliminate the aggressive inclination of human beings. Many other psychoanalysts have made contributions to large group psychology without, however, bringing more comprehensive or satisfactory explanations than Freud’s.
Fortunately, new efforts have been made. In 1978, Egyptian president Anwar-El-Sadat directly addressed and welcomed mental health professionals to work jointly with diplomats in an effort to understand and destroy the psychological barrier, which, in his words, constituted 70% of the problem between the Arab-Israeli people.
A grant was obtained from the United Nations Fund for this purposes and a small committee was created within the American Psychiatry Association, which held meetings in various places in Europe. From 1980 to 1986, Egyptian, Palestinian, Israeli, and American psychiatrists and diplomats split and joined small discussion groups as a way to facilitate the dialog between the parties of the dispute.
This effort brought new and valuable insights into both the behavior and the identity of emotionally linked large groups.
PSYCHOLOGY AS A MEDIATOR OF INTERNATIONAL CONFLICTS
Volkan reports a few interesting facts that occurred at these meetings. In his judgment, nothing was ever made of the ideas discussed. However, these ideas have undoubtedly affected and are still to affect top decisions on the Arab-Palestinian conflict. The meetings have, at the minimum, served the purpose of promoting some long-lasting relationships between the participants as well as of expanding the dialog.
In the beginning, both the Israelis and the Arabs seemed to be in competition as to which of the two had been victimized by more aggression and injustice, and any new incident would rekindle memories of incidents that sometimes dated back centuries.
The grief of one group would create little empathy in the other group and talking about past injuries seemed to enhance the persecution in the present, allowing a sense of group identity to grow.
A crucial moment in the discussions was reached in a small group in which the participants came to the conclusion that both sides shared a feeling of fear. The mutual recognition of fear contributed a positive atmosphere to the discussions. But that only happened following a tense argument between an Egyptian journalist and historian and an Israeli infant psychiatrist.
The psychiatrist asked the journalist how he could ever convince her not to fear the Palestinians. He replied that he found it impossible to believe that the Israelis could fear the Palestinians.
The next day, the journalist said that, unable to sleep all night, he had consulted the Koran and found a passage describing the fear of Moses. Stricken by surprise, he then apologized, saying that “if Moses could have been afraid, she, as a human being, might feel that way as well”.
Another conclusion arising from this meeting was that group mourning was a totally unknown phenomenon. When facing an individual loss, there is a whole path taken by an individual, with the support of a group closely related to him/her, in elaborating feelings of impotence, anger, humiliation, etc., so that he/she may grow to accept the loss and the life change such a loss may impose.
With respect to groups and communities, there seems to be no elaboration of this group mourning to the extent to which a phenomenon Volkan calls a “time collapse” may occur, whereby a trauma experienced centuries ago seems concomitant to a recent event. While both events are intellectually separated, emotionally they move along together.
CULTURALLY UNRESOLVED MOURNING AND ITS TRANSGENERATIONAL CONVEYANCE
Losses experienced by a culture as a whole, such as the killing of beloved idols, natural disasters resulting in a high number of deaths, domination, imprisonment, humiliation of a group by another, etc., also require a process of mourning and elaboration, and an unsuccessful attempt to achieve this may cause them to become perennial.
A culture conveys its message of grief in most peculiar ways. For instance, it may use mass communication to report an event or create anecdotes as a way of elaborating a tragedy. It may use cultural rites for celebrating the anniversary of these traumatic events or it may build monuments of metal or stone to symbolize the strength with which these events will be forever remembered.
Whenever a whole generation is decimated, subjugated, and forbidden to cry and ritualize its loss (as in the case of the Holocaust in World War II and of the Navajos, who were expelled from their land by American settlers in 1864), those surviving such a tragedy are entrusted with conveying their sentiments to their descendants, as if posterior generations could be entrusted with the task of mourning and elaborating once forbidden to their ancestors.
To a certain degree, nothing is ever forgotten by a culture. One could analogously speak of a collective unconscious according to Jung[5] or of a co-unconscious[6], recalling Moreno, or even of post-traumatic stress disorder[7]. In short, there are group mechanisms used for damming up and transgenerationally conveying, in a way yet unknown to science, the resentment, traumas and injustices experienced by a given generation.
Anne Ancelin Schützemberger (1997) presents numerous clinical samples of what she calls the “anniversary syndrome” where within the same family, a given tragic event, for instance, a fatal accident, is repeated for various generations, always on the same date. Another interesting report of hers is about “family secrets” which return encrypted in a given patient elected in a posterior generation who, through his/her symptoms, speaks of what was once before unspeakable and unthinkable.
Ivan Boszmormenyi-Nagy (1983) introduced the brilliant concept of “invisible loyalty”, arguing that family and cultural relations included a dimension of both the justice and equity present within a family or a culture. Symptoms and repeated patterns are means of desperately seeking the restoration of an ethics of transgenerational relationships.
The concept of parentification also comes from this author — the inversion of dependencies in which children take care of their parents. This involves an implicit and complex system of merit and debt bookkeeping in which all that was once received by a child in the form of care, kindness and companionship must eventually be repaid to the parents.
Every injustice suffered by the family will also be entered in the bookkeeping and each family member will be entrusted to the task of either seeking revenge or forgetting injustice. There is no way to escape these family obligations without carrying a feeling of “amorphous, indefinable existential guilt”.
It is interesting to note that, although the word loyalty derives from the Latin word legalitas, which refers to law, its real meaning is connected to an invisible, interweaving of family expectations not always manifested through justice or legality. Individuals who do not learn the meaning of justice within family relationships will tend to develop a distorted idea of social justice.
GROUP NARCISSISM, RESENTMENT, REVENGE AND FURYWould it be possible for us to consider the existence of a narcissistic group system in which individual worth is connected to the worth of the group to which the individual belongs and, as a consequence, that any attack to this group’s self-esteem would trigger responses of fury and revenge aimed at restoring the group’s lost dignity?
We know that this is true on an individual basis. I myself (Cukier, 1998) have previously affirmed that “children abused in their childhood are like time bombs” in that they will seek retaliation for this abuse as soon as they have the power to do so.
In large groups, it seems to take the parallel occurrence of many factors to culminate in a reaction of revengeful fury. The presence of a fanatic leader, with a childhood history of abuse and negligence, is one of these factors. Alice Miller (1993) demonstrates that, behind all great catastrophes of mankind, there were always narcissistic, sadistic leaders hurt by negligent and abusive parents who were never able to deal with the basic needs of their children. This was true for Adolf Hitler, Stalin and Nicolae Ceausescu who were spanked and humiliated in their childhood.
Another predisposing variable is the present occurrence, or a still-remembered past occurrence, of an attack to “the group’s pride”. According to Kohut (1988), group cohesion is achieved through shared greatness; groups will present regressive, narcissistic transformations every time this greatness is attacked. These regressive transformations of group narcissism encompass narcissistic aggression, anger, fury, and revenge. Kohut says:
“The desire to make a passive experience into an active one, the mechanism of identification with the aggressor, the sadistic tensions preserved by those who, as children, were sadistically treated by their parents — all of these factors — help explain the promptness of a shame-prone individual to react against a situation which he may potentially provoke by using a simple remedy: to actively (and often anticipatory) inflict on others those narcissistic damages which he himself fears to suffer”.
There are also culturally rooted factors favoring aggressive reactions, such as symptoms of self-repudiation or shame. This is true for Japanese people who reject the facial characteristics of their own race and undergo plastic surgeries to acquire the characteristics of the majority group in possession of the social and economic power.
Hugo Bleichmar (1987) calls these identifying objects or traces which we wish to possess so that their intrinsic worth may be conferred upon us (such as cars, jewelry, a certain type of eyes, etc.) “narcissistic possessions of the ego”. Bleichmar also shows us how culture has many different terms for reality, which carry identifying beliefs and attributes which confer worth upon an individual. That is true with possessive adjectives used in the context of genetic family inheritance. The words “my, thy, and ours” literally build a bridge between objects and their possessors. Bleichmar affirms:
“The word my comes across to a child as having the same meaning as when used by his parents in my child: the parents’ narcissism requires that the child-phallus be regarded as a product of their own. Therefore, my child stands for the child who, having been created by me, is my own. Hence the expression speaks of myself. ”
Moreover, there are logical rules in the individual unconscious, for instance, the logic of the class structure, which gives equal identity and worth to those included. That is how we understand why, despite impetuous fights within the same family, every time somebody from outside the family criticizes one of its members, because this member is considered the narcissistic property of the ego, all the other members will immediately come to his defense.
To Anne Ancelin Schützemberger (1997), group resentment is a phenomenon connected to the injustice suffered by that particular group on behalf of one of its members. Loyalty as a moral obligation makes all individuals in a group feel they have an obligation to seek equity and justice; whoever fails to fulfill this obligation will be found guilty and deserving of punishment.
“An eye for an eye, a tooth for a tooth” — is the law of Talion [8] , which sets the rules for the final settlement of debts for long-suffering mankind. In the end, we may all end up toothless and blind. Would Moreno be able to help us?
Moreno’s suggestions for treating mankind:
Moreno created sociodrama for treating groups and collective problems. His book ” Who shall survive? “ is wholly targeted at formulating and testing ways to make this project feasible. He defines sociodrama as:
“a deep action method dealing with inter-group relations and collective ideologies” (1978, p. 87)
Moreno made many attempts at theorizing on group behavior. He proposed a distinction between the identity process and the identification process. In his words:
“Identity should be considered apart from the process of identification. It develops prior to the latter in the infant and it operates in all inter-group relations of adult society. For the infant, “self” and immediate milieus are the same thing; there is no self-other relation. “Self” and “other” are two as yet undifferentiated portions of the “matrix of identity” (1975, p. 381).
Moreno suggested the term “identity of role”, for naming what we would contemporarily call ethnic identity:
“Negroes take themselves as a single collective, the Negro, a condition which submerges all individual differences […] We shall call this identity, the identity of role” (1975, p. 442).
Moreno spoke many times of catharsis in sociodrama and catharsis in psychodrama, emphasizing that in sociodrama one seeks to treat questions related to the identity:
“The protagonist on the stage is not portraying a dramatis personae, the creative output of a mind of an individual playwright, but a collective experience. He, an auxiliary ego, is an emotional extension of many egos. Therefore, in a sociodramatic sense, it is not the identification of the spectator with the actor on the stage, presuming some differences between him and the character which the latter portrays. It is identity. All Christians, all Negroes […] Every Christian is, as a Christian, identical to every other Christian […] In the primary phase of collective identity, there is no need, therefore, for identification. There is no difference between spectators and actors; all are protagonists” (1978, p 365).
Moreno did not address group narcissism, but came close when he affirmed that envy could be a resentment engine acting between groups:
[…] “The Jewish population in Germany may have produced more individual leaders than their numeric proportion, either because the Jews suffer from a surplus of leaders or because Germans suffer from an insufficiency in leader production […] As the majority of the dependent groups are Germans, we can imagine feelings of resentment arising among the German leader groups, together with the conviction that they have more “natural right” than the Jewish leaders to direct the German masses of workers and farmers (1978, p. 563).
Besides this, the sociometric test itself, through its calculation of choices, rejections, and neutralities, ends up addressing the narcissistic question at its core, provoking reactions — many times catastrophic — which Moreno pointed out and attempted to explain. On sociometric procedures, he affirms:
[…] “Sociometric procedures should be greeted favorably as they aid in bringing to recognition and into realization the basic structure of a group. But such is not always the case. They are met with resistance and even hostility by others…” (1978, p. 94).
“Other individuals also showed fear of the revelations the sociometric procedure might bring. The fear is stronger with some people and weaker with others. One may be most anxious to arrange one’s relationships in accord with one’s desires; another may be afraid of the consequences […] These and other remarks reveal a fundamental phenomenon, a form of interpersonal resistance, a resistance against expressing the preferential feelings which one has for others” (1978, p. 585).
Moreno was always concerned about racial conflicts and even formulated the idea of a racial quotient:
“From the social interaction of the members and from their emotional expansiveness, a group expression reaches its saturation point for a certain contrasting racial element; this is a racial quotient” (1979 p. 410).
Moreno also formulated the concept of the point of racial saturation in which he expresses the idea that there is a certain point beyond which a majority population becomes saturated with a minority population, which thereby favors racial discrimination:
“A population may become saturated with a minority group at a given time. If an excess of the minority group move into the majority community, the delicate balance begins to break. In the case of a chemical solution, its point of saturation for a certain substance may change with, for instance, the rise or fall of the temperature. In the case of social groups, the point of saturation may change with the organization of interrelated groups.” (1978, p. 721).
In The Negro-White Problem: a psychodramatic protocol, Moreno (1977) daringly discusses the situation of African Americans in the United States, developing some important theoretical considerations on the processes of racial discrimination and the counter-responses it gives rise to.
Actually, after he wrote The words of the father, Moreno seemed to have the firm intention of, instead of pulling out eyes and teeth, as proposed in the law of talion, only exchanging eyes and symbolically exchanging places with and understanding “the other, the enemy, the different”. That is what he does in his “Nazi Prayer” as he shows himself capable of exchanging roles even with the enemies of the Jewish people where he himself belonged:
“Oh God,
Our race is like healthy green grass.
Other races are like weeds,
They hinder the healthy green grass
From unfolding
Uproot the weeds
And destroy them!” (1971, p. 276)
His conceptualization of axiodrama, a sociodrama focused on matters of ethics and value, also denotes a concern with the community context in that it proposes discussing and role-playing the so-called “eternal truths”, such as justice, beauty, truth, perfection, eternity, peace, etc.:
“The organism in the field becomes the actor in situ. Whole cultures can be “acted out” piecemeal in the experimental settings of axiodrama and sociodrama, with the protagonists as creators and interpreters” (1978, p. 61).
Moreno was very deeply plugged, into his time, though also deeply critical of the achievements of his time. For instance, he used to disqualify our over-robot-filled age with lots of technical devices for lacking life and spontaneity and substituting human relationships. However, he did not hesitate to use this same technology in spreading his sociocratic methods. He made use of movies and suggested, in a chapter written in co-authorship with John K. Fischel at the end of his book Psychodrama, possible ways of adapting spontaneity methods to television resources:
“These odd enemies are technical animals, which can be divided into two classes: cultural conserve and machines. The more popular word for them is robot.“ (1978, p. 600)
“It is advisable to organize psychodrama sessions to be broadcasted to the world from TV stations […] It is advisable to organize live and role-played newscasts that can be transmitted to the world through TV stations. This is healthier than the usual photographic newscast of events; it is a tool through which the lively and creative genius may, in this planet, communicate directly and instantaneously with its peers” (1977, p. 419)
Moreno was against dolls, mechanical toys, aseptic baby bottles — in short — against technology. I, however, keep thinking that, were he still among us, he would undoubtedly find a way to use the Internet as a forum for discussions, a free tribune, and perhaps role-playing via satellite, making it possible for archenemies to exchange roles, or find that fear, pain, horror, loneliness, humiliation, pride… — all of these – are attributes shared by mankind as a whole and not only by a particular tribe.
CONCLUSION
I would like to close this paper by paying tribute to those colleagues among us who have put forth their best efforts in pursuing Moreno’s sociocratic lead. I am talking about the growth and creativity of various groups and schools of Spontaneous Theater, groups doing sociodramatization work with rural communities, needy populations and with minorities discriminated against on account of health problems and poverty, and about the growth community services dealing with domestic violence.
I am also enchanted with the possibility of using role-playing as a means for working with large groups. To summarize, I believe that we psychodramatists have the daring that it takes to push this social project forward.
I mentioned daring because a job like this does indeed require a great deal of courage. Volkan (1997), with his group of diplomats, politicians, historians, and psychoanalysts was able to hold few and small verbal meetings, all closed, with a restricted audience. Reading his book gives us a measure of how tense and dangerous the environment in these meetings can be.
Could you imagine ethnic confrontations on TV, all conducted by a skilled psychodramatist, with millions of people inter-acting, sending in questions, contributing arguments, facts… I am amazed by the thought of it!!
However, how many of us would have the audacity to conduct such psycho-political sociodramas? Directing sociodramas and large audiences is a task very few would be able to perform. In fact, no psychodrama school has ever prepared us for such a task. Moreno gives us an idea, but we have a lot to learn.
I have already witnessed chaotic sociodrama sessions with directors lost and ashamed — and I have even watched shoes being thrown by an enraged audience. Large groups, such as described by Freud, seem to function like a wild animal in need of taming, and words, as used in individual communication do not convey their messages in the same way. Maybe applause or cheers would do the trick… Maybe we should seek the help of mass communication professionals.
I do not know exactly how to go about it, but I have a feeling that we must learn in a group how to deal with groups. The experience of studying Moreno – such a complex writer and author — with GEM[9], in a group, bit by bit, patiently and persistently, has taught me that everything is possible whenever a large number of people are working together.
In closing, I would once again like to remember Volkan’s (1997) suggestion, that maybe it is necessary to articulate great intercultural, intergenerational, and multigenerational apologies. Not long ago we watched Mikhail Gorbachev apologize on behalf of Russia for the massacres in Poland. the Catholic Church has also apologized for its apathy toward the extermination of Jews during World War II.[10]
I wish Moreno could accept my apologies for the many times I regarded him as a foolish dreamer, alone up in the hill, looking at a future only he could glimpse at. Maybe he was indeed a fool — but he is not the only one. There are many fools like him trying to help the United Nations so we can at least have A FUTURE.
References
- Bleichmar, H. (1987). O narcisismo. Estudo e Enunciação da Gramática Inconsciente Editora Artes Médicas, Porto Alegre , Brasil.
- Boszmormenyi-Nagy I. (1984)- Invisible Loyalties : Reciprocity in Intergenerational Family Therapy , Brunner/Mazel, U.S.A
- Cukier, R. (1998). Sobrevivência emocional: as feridas da infância revividas no drama adulto, Ágora. , S.Paulo-Brasil.
- Décio de Freitas (1998). Máscaras do neo-racismo, Jornal “O Globo”, 9 de agosto de 1998, Porto Alegre-Brasil.
- Freud, S. (1920-1921)- Psicologia das massas e análise do ego. In – obras completas, tomo III , Editorial Biblioteca Nueva, Madrid.
- Kohut, H. (1988). Psicologia do self e cultura humana., Artes Médicas. Porto Alegre-Brasil.
- Miller, A. (1993). Breaking down the wall of silence. New York, Meridian Book.
- Moreno, J. L (1977). Psychodrama. vol. 1, 4th ed., New York, Beacon House.
- Moreno, J. L. (1971). The words of the father. New York, Beacon House.
- Moreno, J. L. (1978). Who shall survive? Foundation of Sociometry, Group Psycotherapy, and Sociodrama, New York, Beacon House.
- Samuels, A. (1988). Dicionário crítico de analise junguiana.. Imago. Rio de Janeiro-Brasil
- Schützemberger, Anne A. (1997). Meus antepassados. Paulus Editora, S.Paulo-Brasil .
- Volkan, V. (1997). Bloodlines: from ethnic pride to ethnic terrorism., Farrar, Straus and Giroux,. New York.
- [1] A major armed conflict is defined as a prolonged conflict between military forces from two or more governments resulting in over 1000 deaths.
- [2] Terrorist attacks inspired by ethnic and/or religious differences and led by individuals and small groups.
- [3] The difference between a nation and an ethnic group is that the idea of nation implies political autonomy, the establishment of frontiers or, at least, organizations establishing roles, positions, and status. The majority of nations are formed by more than one ethnic group and some researchers call these ethnic groups sub-nations.
- [4] In Yugoslavia, for instance, it is people of the same blood but of different religions who kill one another
- 21Jung’s collective unconscious is a broader concept than Freud’s concept of the unconscious. Jung’s concept includes, besides the repressed childhood experience, the experience philogenetically accumulated by mankind, which functions independently from the Ego because it originates in a structure inherent to the brain. Its manifestations are found in culture in the fashioning of universal motives, which possess their own degree of attraction.(Samuels 1988))
- 22 Moreno(1975) describes the co-unconscious as a state shared simultaneously by all participants of the same living experience and which, therefore, can only be reproduced and represented by a group.
- 23 Post-traumatic stress disorder consists of a debilitating reaction following some traumatic event. Very frequently encountered in war veterans, it also includes reactions to serious accidents, natural disasters, and violent assaults such as rape and torture. The onset of this condition causes a person to have recurring memories of shocking facts, which intrusively devastate their thoughts in the form of nightmares or of daytime fantasies. Sleep disorders, irritability, the lack of a sense of belonging, and loneliness are also experienced.
- 24 The law of talion [lex talionis], which belongs to the Code of Laws of Hammurabi, King of Babylon in 2500 BC, by which a penalty inflicted should correspond in degree and kind to the offense of the wrongdoer.
- 9 GEM – DAIMON – Group of Studies of Moreno’s Works at the Daimon Clinic in São Paulo
- [10] Today (feb/17/ 2000), as I ‘m revising the final version of this article for the “Forum” , I’m deeply touched by Johannes Rau, Germany’s president, who apologizes the Jewish Community for Holocausts .
-
THE PSYCHOSOCIODRAMA OF ENVY: WHO WANTS TO THROW THE FIRST STONE!
Introduction
I have never been able to cope with the emotional experience of[ii] envy. Neither my own, horribly embittered inside my thoughts, and nor the others, wisely denied and exteriorized with touches of resentment and rejection.
After reading a vast amount of literature over the last few years, I perceived that, of all human life experiences, Envy is the least studied and about which the least was written, especially in psychology. Only human sexuality had been repressed so much in other times.
Some authors say that there is no dignity in such a feeling. Even extreme rage and hatred may be explained by any noble reason, but Envy always represents an obscure feeling, without legal justification, mean and isolated, futile, hidden as it best suits bandits, thieves and assassins, the scum of human race.
And, however, throw the first stone if you have never felt it, and if you have never wished someone evil based on an attribute you admired, and if you have never avoided situations in which you had to confront people exhibiting qualities that you lack, and if you have never sided with someone just to favor those who possessed aspects you coveted, etc. Practically everything that brings happiness stimulates envy” says Aristotle [1].
And perhaps you may also have never thought that without Envy, and the consequent capacity of always being comparing and watching ourselves mutually, we wouldn’t have the development of social systems to which we all belong and in which lies Envy, sovereign, like a drab eminence, behind social and economic policies and almost all revolutionary movements of the history of mankind.
According to Helmut Schoeck (1987) [2] there are crimes caused by envy, policies based on envy, institutions meant to regulate envy and numerous reasons to avoid being envied by others.
Molded in a feeling of injustice by differences (whatever they might be: financial, aesthetic, philosophical) and in the idea that everyone should be equally favored, many policies of expropriation were conducted. From the XVIII century, with the emblematic motto of the French revolution “equality, fraternity and freedom” until the socialist revolutions (XIX and XX centuries) this philosophy of equality is proclaimed an opium for the feeling of envy, which gains demagogic strength in this apparently fair indignation.
According to de La Mora (1987) [3] Envy is the biggest unspoken human taboo; everyone feels it, but a few admit it, which makes its study hard and indirect. Curiously however when honorably vesting this ideological carcass of equality, it becomes the bastion of human justice. The same author concludes in his bright book ”Equalitarian Envy” arguing for the healthy necessity of the difference, and for the absurd of one’s imagining that equality may be conquered by coercion or demagogy.
Just out of curiosity and already approaching psychology and psychodrama, we know that Envy is a feeling apprehended in cluster one and massively externalized in cluster three (Bustos: 1994-362)[4], cluster of symmetrical, fraternal and amorous roles, with the dynamics of cooperation, competition and rivalry .We do not usually envy kings and queens and their fortunes accumulated without manual work, but we may envy our next door neighbor, because he bought a brand new car. Cain and Abel’s history appears to be the right metaphor to illustrate this sentiment.
Well, we are all different. And we have to learn how to cope with these differences. Is ever it possible? How can we learn to deal with the differences? How can we better live with the primordial injustice of the human existence? What to do when I feel envious? How to cope with other people’s envy? Have I really provoked their envy? Can someone who envies cause me any harm, the famous “evil eye”? These are the questions that make me research this theme. That’s why I also propose the Psychosociodrama [iii]of Envy, in the hopes that we do not remain silent over shameful themes, but, on the contrary, respectfully united follow this arid path.
ENVY: THE CONCEPT
“The number of those who envy us confirms our capabilities”.
The word envy comes from the Latin In- videre, which means at sight, that is, being seen. Envy manifests itself popularly through the evil eye, the devil’s eye. To be seen seems to be essential to the Envy theme, either to those who are envied (they are seen) or those who envy (they see). This psychological phenomenon presupposes a social context: the co-existence of two people.
Numerous definitions of this feeling range according to the aspect of the phenomenon we want to tackle:
- Envy is a kind of psychological pain felt when comparing ourselves to other people, we conclude that our value, self-esteem and our respect are diminished.
- Envy is a painful observation of what we are lacking..
- We feel envy when another person has characteristics that are superior to ours.
- Envy is a type of admiration and love for something we lack.
- Schadenfreude is a German word also used in other languages to designate the feeling of joy or pleasure for the suffering or misfortune of the others.
- Envy is a feeling that invades us when we observe other people’s success.
In all languages, from the primitive ones to the Hindu-European, Arabic, Japanese, Chinese there is a term that designates an envious person. The primitive polygamous societies already had policies to deal with envy, especially related to the distribution of affection and goods equally among wives and descendents. A lot of conflicts took place due to inequalities and a lot of superstitions were created in order to magically obtain the desired benefits. (Helmut Schoeck3).
Envy is therefore a universal phenomenon and the literature, religion and philosophy are full of studies and metaphors on this subject. Look at the following:
- “Because he possesses herbs and grains…he is envied by the Philistines”. (Bible -Genesis 26:14-15).
- “Envy sees only the bridge, not the span that covers it”; “For envious eyes, a mosquito becomes an elephant”; Envy sees the ship quite well, but not the hole in its hull, (Russian literature).
- “Fear Allah and do not envy his power”.” Envy devours faith like fire devours wood”. (Islamic literature).
- “Envy is the pain caused by the good fortune of the others” (Aristotle, Rhetoric , book II, 10).
- “Envy wishes to destroy the good fortune of the others”. (Kant, Metaphysics of Moral .6: 459).
- “Envy is the passion that sees malign displeasure the superiority of those who have the capacity to deserve the superiority they possess”. (Adam Smith, The Theory of Moral Sentiments, p. 244).
However, to conceptualize this feeling is not an easy task; one can confuse it with the complex feeling of jealousy and this discrimination must be done. Another difficulty emerges from the possible gradations of this feeling. It is then that we hear about good envy, very close to admiration and easy to be admitted, in opposition to “bad envy”, which is really similar to the German word Schadenfreude, consisting of a real torment before the good fortune of the others and an extreme pleasure in their misfortune.
ENVY & JEALOUSY
«Jealousy fears to lose its possessions; envy suffers watching the other having what it wants for itself”
It is not always easy to separate envy from jealousy. Both feelings presuppose social interactions, comparisons among individuals and are extremely harmful for the relationships.
Envy generally refers to a dual relationship[iv], in which the subject misses something the other possesses and wishes he wouldn’t have it. Whereas jealousy has to do with triangular relationships and basically consists of the fear of losing a relationship for another person. Envy prefers to destroy while jealousy aims to control.
A flaw can be found in both feelings. In jealousy the flaw refers to the fear of losing something or someone who is already yours to somebody else. The flaw in envy refers to something that you don’t have, but the other person does.
Both feelings are externalized very similarly: they are partly denied, but appear indirectly under the fear of losing, rage, cheating, insecurity, inferiority, vengeance, paranoia, etc.
Foster (1972: 167) [5]suggests that envy provokes jealousy as a counter-reaction, as if they complemented one another. For instance, if someone feels that his beautiful wife is being coveted, he becomes jealous fearing to lose her. The same happens to any object or attribute that is wanted. He who has something does not want to lose it, and he who does not possess something wants to get it, at least, does not want the other to have it.
GOOD ENVY & BAD ENVY
Maybe to minimize the impact of such a shameful feeling, or to dialectically avoid the false polarities between good and bad, some authors argue that envy has at least one positive factor, since it can be the fuel or an extra motivation to reach success or acquire attributes leading to happiness.
For Carl Gustav Jung [6] analytical psychology, no matter what trace of character or attitude exists in the conscious and dominating mind, its opposite equally reigns in the unconscious. The repressed content in the unconscious must become conscious in order to produce a tension of the opposites, and thus make the personality flexible and enrich it. Says the author:
“All this process is called “transcendent function”. It is at the same time a process and a method. The production of unconscious compensations is a spontaneous process, whereas the conscious realization is a method. The function is called “transcendent” because it favors the passage of psychic constitution to the other, through the mutual confrontation of the opposites (JUNG, 1991, p. 15)”.
Byington (2002: 21-22) [7] talks about the creative potential of Envy, which would be only one of the structuring functions of the Psyche, being able to act creatively and provide the healthy development of the personality or, on the contrary, become fixed and begin to act in the Shade[v]·, in an inadequate, repetitive and destructive way.
In an article about the work of Gonzalo Fernandez de La Mora (1987) “Equalitarian Envy”, the author Eduardo O. C. Chaves (1991)[8] shows that, in view of the possibility of the others becoming happier than us, it is possible to assume one of the three attitudes:
- a) Emulation- The desire to be like the others, act like them, and possess the things they possess.
- b) Resignation- To accept our (real or supposed) inferiority.
- c) Envy- To wish the others lost what they have and wish it were ours.
The attitude of emulation is positive; it triggers progress and human development. The more it stimulates competition, the better. Fernández de La Mora says: “Do what you have to do, and do it better than anyone else”− referring to sports in general, which wouldn’t have progressed had people not tried to improve it.
The attitude of resignation may have negative and positive aspects. It is negative because as the subject resigns he fails to contribute for the progress and human development, leading to stagnation. It does not promote involution, though.
The attitude of envy, however, is just negative because it leads to involution. The envious individual wishes misfortune and misery to those he envies; he wants to see those superior to him reduce to his level.
Briefly, I think that it is possible to use envy as a catalyst of energy toward envied objects, more or less like a plan of life or ambition. This would be the good envy, the emulation that causes no harm to anyone, neither to those who try it nor to those serving as its target. To admit it would do good to the self in the sense that Kohut[9] meant to affirm: “we are pushed by our ambitions and led by our ideals”.
However, the focus of my paper today is not this benign envy, but the other one that makes you suffer by the impact of observing other people’s attributes that point to our own inferiority and ends up in a personal impotence and desire to destroy the other. My focus is the so called “Green Envy”, a term coined by Shakespeare in Othelo[10], referring jealousy, probably an allusion to the hepatic bile, a viscous digestive yellowish green secretion produced by the liver and as bitter as this sentiment.
ORIGINS OF ENVY
“When one of my friends is successful, something dies inside me”.
Gore Vidal
Why are some people more envious than others? Is envy inborn or is it learned? The The origins of envy are debatable. The Freudians, led by Freud and Melanie Klein, associate envy with the death pulsion, whose origins would be innate. Freud in 1908[11], in his article “The Sexual Theories of Children” mentions the interest that girls have for the penis of the boys, interest guided by envy. But only in 1914, “Introduction to Narcissism” [12], he coined the term “penis envy”, designating the complex of castration in a child of the female sex. In 1920[13] with the publication of “Beyond the pleasure principle”, Freud postulates that functioning of the psychic apparatus is based on the opposition between two basic pulsions: life and death. The pulsion of death would be omnipresent, would appear generally merged with the pulsion of life, and would manifest itself in various ways, such as: compulsion to repetition, negative therapeutic reaction, aggressiveness, envy, destructive narcissism, etc.
For Melanie Klein (1974)[14], the origins of envy are innate and derive from the constitutional aggression. An excessive load of precocious envy represents a particularly malign and disastrous form of innate aggression. Primarily, the child would be envious of the breast, and later, and by displacement, she would encompass the breast-penis equation, symbols of life. With a greater integration of the self and the appearance of guilt and the desire of reparation, envy tends to give in to gratitude. Whereas envy spoils the fruition of the object through the desire to destroy it, gratitude is the contrary “… the fundament of the appreciation of what is good in the others and in himself ” (Cintra eandFigueiredo, 2004, p. 133) [15].
The neo-Freudians like Karen Horney and Winnicot, emphasize less the importance of biological forces over the personality, and highlight the impact of social and psychological forces. They also minimize the importance of infantile sexuality and Oedipus’ complex, suggesting that the development of the personality is determined mainly by psychosocial forces and not psychosexual ones.
Karen Horney[16] argues that the “penis envy”, as described by Freud means only envy of masculine power in the patriarchal societies. She proposes the concept of the”uterus envy”, suggesting that men would envy the feminine capacity to generate lives.
Winnicot[17] believes that the newly-born does not experience – by nature – any overflowing or pulsional conflicts; he only has basic needs that have to be met by a good enough mother.
Dave Hiles [18], a psychotherapist of the Tavistock clinic, revisits the Kleinian theory and translates it in light of the love and hatred dynamics in the relationships. The human child is born in a state of semi-parasitism, totally dependent of her caretakers, especially of the mother who feeds her. All her action and reaction are directed to have her mother for herself, including her reactions of hatred,; this would be a form to draw the mother’s attention and have her around to manage to survive. The child does not want to destroy mother, but control her presence absence.
For him, envy is not a gratuitous aggression towards everything that’s good, but the fragile response of the child before privation, the belief that what he needs is being refrained by someone who does not to give it to her. The resulting rage would be an effort to induce the mother to realize her desires, not to destroy her. He cites Ian Suttie[19], a Scottish psychiatrist, prior to Melanie Klein, and inspirer of ideas of Bowlby[20], who contested the Freudian sexual theory, and for whom the greatest challenge of the human development is to become independent of the mother, and rage hatred, jealousy , envy take place when this challenge is not reached.
EVOLUTIONARY FUNCTION OF ENVY
From an evolutionary perspective, envy is seen as an important instrument in the struggle for a competitive advantage (Hill & Buss, 2006) [21]. The basic concept of Charles Darwin’s Theory of Natural Selection is that favorable characteristics that are hereditary become more common in successive generations of a population of organisms that reproduce themselves, and that unfavorable characteristics, which are hereditary, become less common.
The process of natural selection is inherently competitive. The primitive man struggled for food, shelter, warmth and, if someone had these resources and he didn’t, he would do anything to obtain them, on the account of his survival. We are phylogenetically equipped, in order to observe us and compete, and we manifest these attributes in our social interactions. We continuously struggle to acquire resources or positions that the others simultaneously are struggling to get. This occurs with the physical appearance, as we acquire perishable goods and even when we profess ideologies, beliefs, etc.
The use of social comparison is a survival instrument through which men can evaluate if they are at advantage or disadvantage in the battle of natural selection. Therefore, envy would serve the function to warn when a rival partner is at an advantage and would push the individual in question to try and get that advantage for himself.
The negative affection felt when one perceives the advantage of the others, say the authors, results from an internal alarm that signals that we are losing the competition (which, in primitive times, would mean death for us and our offspring). People feel rage, pain[vi],[vii],[22],[23]and shame as I will mention later, as if an injustice were happening and try to re-establish their well-being in several ways. Many friendships are broken because one of the partners is at disadvantage and prefers to keep away form this feeling.
To keep envy in secret is also a defense strategy, since admitting it may only maximize other people’s merits and would make it impossible to use other strategies, like gossiping to demoralize the other, and say it was unfair, etc.
WHEN DOES ENVY TAKE PLACE?
Every explanatory theory about envy has its way to predict when an episode of envy will take place.
Psychoanalysts, in general, believe that envy is directly related with the experience of primary child care. That is because the sense of having attributes, commonly called self-esteem, is opposed to being completely impotent, without attributes, without self-esteem.
A Klenian therapist Kate Barrows (2002: 65-67) [24] says that envy occurs more often in certain types of relationships, in which questions related to how things are given and received are raised. If a person giving something does it in a cordial way, without belittling or humiliating, the person receiving tends to feel grateful and will return something out of gratitude. On the other hand, if the person giving does not like to do it or makes it clear that he is only giving because the other person wants it, this individual will feel offended, resented, inferior and may become envious. The individual does not fee free to appreciate what was given to him.
Richard Smith (2004) [25]in his brilliant article “Envy and its transformations”, summarizes the four conditions for envy to take place:
- Any envy episode starts with the observation of an attribute in another person that we wish to have.
- The envied person is symmetric to us in many aspects: age, socio-economic level, etc. This similarity generates a sensation of injustice, “ if we are equal, we should have the same things”.
- The attribute that the other possesses is of a relevant domain for us.
- Our personal perspectives to obtain this attribute are very scarce.
To summarize: we want to have what the other person has, what our basic similarities suggest that we should have and what would fair for us to have, but we come to the conclusion that it is beyond our reach. All these characteristics are necessary for the onset of envy. If, for instance, the object of comparison is not relevant to us, we may admire it in the other without feeling the pain of envy; if there is a low similarity of attributes, for example, the person we look up to is older, we may think reasonably that when we grow older, we will also have that quality. If we believe that we are able to get that quality, we will fell motivated and we will struggle to obtain it and, again we won’t feel the pain of envy.
Once the four conditions are met, the envy episode will take place, evolve and produce several other emotions (paranoia, resentment, shame) dispelling the initial sensation of envy. For instance, if the focus of comparison is directed to an inferiority of skills, we may feel ashamed of this inferiority, and begin to censure the person in question morally, blaming her for dishonesty. This diverts the focus of our recognized inferiority and justifies our acting malevolently against the envied person. “Merit envies the results”, according to Montaldi’s suggestion, cited by Smith (2004).
Some people, aware of their envy, decide to work hard to make up for a disadvantage and turn it smaller. This is probably the most honorable way to cope with this feeling. Conversely, others remain stuck in the inferiority feeling produced by envy and may fall into depression. It is reasonable to think that a badly resolved envy lies at the bottom of psychopathological cases.
Another configuration that envy might take is the use of slander, gossips, or indirect sabotage to undermine the qualities of the envied person. Gaiarsa [26] (1978) brightly explores this territory and states that chitchat, intrigue, gossip is a means of social control frequently provoked by envy. He dubs “ Emotional Pest”, this subreptitious form used by envious individuals, once they cannot admit their real motivation.
Avi Berman (2007: 17-32) [27], a clinical contemporary psychologist and group therapist of Israel, based on his observation of children, thinks that envy contains a component of hope, a desire to have the same qualities.
This author proposes three factors that may distinguish those who tend to feel resentful and destructive when they are envious from those who find self-accomplishment and motivation in these unfavorable situations. The first factor refers to the awareness of envy and may admit this feeling. The second factor refers to self-esteem and above all to a self-evaluation of one’s own capacities. The third factor comprises how far the person reckons he is entitled to those qualities.
People who benefit from situations involving envy are those who admit the feeling, believe in their capacity and think they deserve it. However, those who suffer with this feeling and become aggressive and destructive are those who do not recognize envy, feel incapable and think they deserve much more than their rivals.
SELF-ESTEEM, COMPETITIVENESS, ENVY AND GENDER.
Competitiveness, self-esteem and Envy appear correlated in almost all the texts that I read for this article. If we think of envy as an adaptive emotion that makes us compete to survive, even so the theorists of the human emotion development had to explain to us how we learn to compete, or yet how we learn to evaluate our real capacities so we can compare with our rivals.
If a person assesses herself wrongly, she will compete wrongly. It is no good to have many attributes if the inner sensation is of depreciation and points toward deficiencies. How do we incorporate the notion of what are our real capacities, our self-value, our self-esteem?
Moreover, each culture imbues its citizens with values that condition the criteria for being accepted and valued or not. Our historically patriarchal culture has changed visibly, but some subtle traces take many generations to really settle down. Carol Gilligan (1982) [28] in her book “A Different Voice” shows that even today there are different competitive forms for men and women. Men are still raised for growing separation from the others and reach autonomy and independence, whereas from women one expects that, above all, they look after the relationships and be friendly and faithful.
If a man is competitive, powerful and well-succeeded, he is still in accordance with the expectations we hold from him, while a powerful, self-sufficient and well-succeeded woman is often threatened to be abandoned by her peers, as if she were a traitor, walking the other direction.
Psychoanalysis also explains this issue, showing that in phases of individuation-separation from the mother toward other relationships and autonomy, boys do not experience conflicts of the kind. If everything goes smoothly, they follow toward the identification with the father and his social roles. The girls, on the other hand, have to individuate-separate from the mother, but at the same time remain identified with their functions and social roles, which presupposes, on the contrary, non-differentiation and intimacy. (Chodorow, 1978, p.109).[29]
To compete with the mother means to separate from the complicity with her, to struggle to become different from her, better than her yet similar is a complex psychological task and carries immense pain and guilt. (Lerner, 1990) [30]. Women permeate their other relationships of the kind with this conflict; that’s why when a woman competes, in general, she seeks a less individualistic and more indirect formula. The win/lose of these situations is based on “everybody wins”, together we win in a team, etc. (Navaro, 2007) [31]. Covered, passive-aggressive styles of fight, modesty and humbleness have been pre-requisites of femininity and to those acting differently, one uses not so noble adjectives, like masculine, aggressive or hysterical. (Lerner, 1990).
And what does envy have to do with this? You must be wondering. Well, if one cannot express openly what he wants and fight openly for what he needs, then he can only envy this capacity in the others. Envy is the best defense mechanism for a self that has been deprived of resources and admires someone who has them. One can relieve the pain of impotence with it, utilizing not so noble hidden attitudes, such as gossip, slander, and anything that weakens his rival.
Although Envy is a universal human phenomenon, and although it affects men and women, it is still more identified as a trace from the feminine culture, and reasonably enough, the witches that were chased and killed in the Middle Age for their evil activity were women.
WHAT ABOUT THE EVIL EYE, DOES IT EXIST, IS IT HARMFUL?
The “Evil Eye” is the belief in which a disease is transmitted – usually unwillingly – from someone who is envious or jealous. This person, normally, is not your enemy, but feeling envious, he/she may harm you, your children, your animals, or your plantation, by casting an envious look. The main victims are the babies and small children because they are very much observed and praised by strangers.
In Hebrew it is “ayin há’ra” (evil eye), in the Italian continent “mal occhio” (bad eye) and in Spanish “mal ojo”. So, there are different connotations for this superstition in every language, as well as records of rituals and amulets for protection in every culture, from the tribal societies to our times of global society. For example, there are reports about envy in the Sumerian writings from 4000 years B.C. (Langdon, 1981) and in the sarcophagus in Egypt in the XXI and XXII centuries B.C. (Rojas- Bermudez, 1998) [32] there are drawings of eyes symbolizing acting and negative energies.
In table 1, as an illustration, I summarized the most frequent intercultural findings:

TABLE 1- ENVY OBJECTS, CURSINGS AND AMULETS
In the Oriental Mediterranean and in the Aegean Sea region, specially in the whole of Greece and even in Turkey, there is a strong tendency to see blue-eyed people as carrying the “bad eye”, probably because few people have blue eyes in these regions.
In Greece and in Turkey, a glass or porcelain blue eye and a Hamsa hand – mystic artifact showing the palm of the hand with five fingers stretched out – are usually displayed in necklaces and in jewelry, as if to face the “blue eye of envy”. In the Christian countries, making the sign of the cross or a “figa” with the fingers (a gesture using a special crossing of the fingers) seems to be the mostly used antidote.
Alan Dundes [33] made a multicultural study of the talismans and healings against the “evil eye” and he noticed common features. It seems that the harm caused by the look is often connected to symptoms of dryness and dehydration, as if the look were a kind of micro-wave and many rituals for the healing usually involve humidity. I concluded that the belief in the evil eye is just another way that human beings have found to deal with the enigma of life and death, consisting of creating metaphors and rituals to keep the living humid in opposition to the dead, dry of all the vital fluids. We can see a typical example in the fish used by the Japanese as antidote against the envy because they are always wet. Also, among the Jew, it is a habit to spit at both sides of the envied person.
For Freud (1901: 919) the belief in the “bad eye” is a superstition and as such, it represents the fear of future misfortunes. Besides, the fear that people “wish us harm” would be the conscious manifestation of the unconscious repression of our own bad wishes against the others. However, it is necessary to remember that despite being superstitious, this belief has the power of suggestion effect that cannot be undervalued.
The superstitions are ideas absorbed from the environment. They are emotionally linked to the potent and primitive tendency, either instinctive or ancestral, of reacting with great fear to everything which may have any relation to supernatural powers. Such tendency, clearly expressed in the child and in the primitive man, continues latent in the civilized adult, being about to emerge in critical situations, even in people with high cultural level.
From Franz Anton Mesmer (1734- 1815) [34] who, using his animal magnetism, healed pains and illnesses by applying magnets to the forehead of people, to Jean Martin Charcot, (1825-1893) [35] the hypnotizer of the hysterical women and Freud – who abandoned the hypnosis concluding that it was just the power of suggestion, culminating with the contemporary Cognitive therapies (Beck and Kuyken, 2003) [36] – we know that the beliefs we have about ourselves, about the world and about the future, determine the way we feel and how we behave, deeply affecting our well-being.
So, yes, “the evil eye” is harmful. Both envied and envious are damaged by believing in this superstition: the envious one for believing that he/she is inferior to the person with whom he compares to and for obsessively losing his/her time and creativity trying to control the envied one. As to the person who believes having been infected by “the evil eye”, will also present, for the power of suggestion, the corresponding harm and will feel impelled to perform a ritual for healing.
MARKETING AND ENVY- THE POWER AND THE DANGER OF BEING ENVIED
Most of the studies about envy focus their observation on the envious person. The target of envy, the person who is envied or who makes himself/herself envied, is scarcely studied. Having qualities, facilities in life, being in an outstanding position cause various sensations, from power to guilt, discomfort and fear that something bad is about to happen.
The Greek, according to Helmut Shoeck (1987: p.141-152), mentioned the Gods’ envy in several myths, as if there were a divine justice in the distribution of wealth with a guaranteed punishment for those who dare trespass the limits. In the same line of reasoning, we can see the idea that the pleasure is prohibited in many religions or at least taxed with the tithing that proceeds with the redistributive justice and still, all the rituals of knocking on wood, making the sign of the cross, etc., each time we realize that something good is happening.
In a capitalist society, where consumption is encouraged by aggressive marketing which overuses the comparison among people, we are instigated to envy something all the time. We envy the car which is attractively offered on TV by a person even more beautiful than the car, who is clothed and accessorized, more beautifully than her and the car and, above all, she is being photographed at a paradisiacal place, much better than the car, the model, the clothes and the accessories.
Being the target of someone’s envy grants this person a status of power and the reassuring of his/her own value. It predisposes him/her to receive aggressive acts, either direct or indirect, such as moral devaluation, gossips, sabotage, etc. and an uncomfortable feeling of guilt for being the involuntary cause of someone’s suffering.
As well as the consumer, target of the advertisement exemplified above, when we are compared to people who have attributes (objects, beauty, quality, etc.) better than ours, we feel attacked in our self-esteem, which demands a retaliation action to recover our value. Making yourself being envied may be an aggressive act, because the envy is a social emotion and affects, not only isolated individuals, but also groups.
George Foster (1972) suggests that there are two ways to analyze envy: from the competitive point of view, it is useful to be envied; as to the point of view of fearing retaliation, it is safer not to be perceived and conceal your qualities.
Dealing with somebody else’s envy is a complex task. The studies in Social Psychology suggest some strategies commonly used to deal with envious people:
- Minimize our own qualities;
- Value the effort we had to make to achieve these qualities;
- Praise the person who envies us, trying to point out his/her qualities;
- Help the one who envies us, trying to give him/her something good;
- Conceal our qualities under a fake humbleness, modesty.
- Socialize our profits, showing how our qualities help other people, etc.
Being envied after all, is an ambiguous existential position. At the same time in which it represents a solitary way of reassuring, surplus value, it may end up producing relationship isolation, lack of harmonious peers with whom sharing joy.
THE ENVY IN PSYCHODRAMATIC LITERATURE
I have found only one text dedicated to envy in our national and international psychodramatic world. It was Rojas-Bermudez[37]’s paper (1997) – “De La envidia y de La violencia”. Bermudez studies the relation between envy and violence, concluding that violence is the result of lack of resources of the Self to elaborate the envy provoked by the other.
He conceives the envy as a natural aspect of the human being, like the fountain and the thirst, but it is insatiable, as a consequence, its tragedy (sic). It is unleashed by a social fact, meeting someone whose virtues make our limitations evident. Says the author: (1997:53)“the envy is an emotional response that emerges due to previous existing lack of affection and that gets established as passion”.
To elaborate further, depending on one’s intra-psychic resources, values and intellectual possibilities transform this suffering in creativity and compensate the lack of affection. If he/she fails, he/she will first try to fight against this passion and later, he/she will cast his/her energy against the source of his/her passion, the other, the envied one, beginning the violence.
Moreno[38] did not directly study the phenomenon of the human envy, he only mentioned it occasionally in his work, although he referred to several questions relevant to the theme, through the sociometric test.
He mentions, for example “the creator’s envy”, referring to the rivalry existing among creative people, either heroes, scientists, or revolutionaries, rivalry that could even be evaluated through the citations the authors of scientific papers make about their colleagues:
… This phenomenon was named “the creator’s envy”. People like him, pioneers of the ones who perform the position of “public-relations” in our illuminated era, may have appeared frequently in the course of history, heroes of the people, acting simultaneously as anti-geniuses and geniuses. … There has often been rival geniuses in conflict with each other; the fire was stolen from each generation and so, gradually the scientific methodology was developed.(he refers to the myth of Prometeus) (1992: v. 1 p. 135).
… I used a cold sociometrics (cold because it is frozen in books).(1992: v. 1 p. 135).
He even seems to believe this competitivity is positive for science, despite being painful for the sociometric stars that may be rejected by their pioneerism. He says:
“the creator’s envy phenomenon also has good social characteristics; it helped the scientific method to be released” (1992: v.1 p.140).
The psychodramatic production revealed intense hostility, being reinforced by one of the two key-individuals and rivals, sometimes resulting in a distorted perception of the pioneer and of his/her work. “The “chain reaction has produced social network denial which may be called antipathy for the pioneer, or ”creator’s envy”. (1992: v.1, p. 136-137)
Moreno also understood the sociometric power of envy, which through direct or indirect boycott, may relegate creative geniuses to ostracism.
… to exalt or to blame, to steal or despise silently, to cite occasionally or not to cite the work of a genius is a dynamic way of determining his/her fortunate career. (1992: v.1, p. 139).
As to social revolutions and their motivations, hidden behind ideologies, Moreno wisely perceived the importance that the feeling of envy has when the disputes involve merit matters versus justice matters[viii]. He says about the Nazism:
… If, as it is stated, the Jew in Germany have a disproportional situation, according to their numerical importance, in liberal professions, in arts, in industry, this may be due to an excessive effort from them, maybe bigger than the effort made by the Germans, equally talented. In this case there are currents both aggressive and protective, in the attempt of balancing conditions that seem to threaten the strength of certain elements from the majoritarian group. (1992: v.3, p. 128).
… As the majority of the dependent groups are German, we can imagine the rage coming up among German groups of leaders, feelings that are joined to the belief that they have more “natural rights” than the Jewish leaders to lead the masses of workers and German farmers. (1992: v.3, p. 130)
From Moreno’s understanding, it was his aim to give relevance to the power a human being has above the other, the importance of being appreciated and accepted, not only in the first affective relationships, but also in all the relationships throughout life. He has always been interested in the rejected minorities, in the sociometric proletariats* (1992: 225) trying to re-integrate them in a certain group. He has done this through sociometry, especially through the Sociometric Test, whose basic proposal was to allow people to choose the relationships and the groups where they wanted to study, work and live.
He did not dedicate directly to the matter of self-esteem or narcissism in any moment of his work. He did not do it probably because of the emphasis he has always given to the relationship aspects instead of intra-psychic matters. The closest he got to reflect the matter of the Self with itself, was the formulation of the concept of “auto-tele” (Moreno, 1992:140) used for speaking about the relationship of the child with itself and with its image, and about the collapse of the psychotics’ self-image.
Sometimes, Moreno seems to refer to the notion of personal value, but the term he uses is “status”. He mentions, for example, “sociometric status” (1974:234-235; 1992 v. III: 194-197) referring to the total of choices the individual has in a group; “status of the men in the cosmic order” (1984: 24) about the commotion the Copernican discoveries represented for men’s pride, etc.
Due to the resistances (1992:202-203) brought about by the sociometric test, Moreno perceives that there is a fear in exposing the relationship preferences. Referring to the sociometric procedures, he states:
“The resistance seems paradoxical at first, since it appears in opposition to the real opportunity of having a basic necessity fulfilled. This resistance of the individual against the group can be explained. It is on one hand, the fear that the individual has of knowing his/her position in the group. Becoming aware of this position, either by himself/herself or through the others, may be painful and unpleasant. Another source of resistance is the fear that it may become apparent to other people we like or even the ones we do not like and which would be the position in the group that we really want and need. The resistance is produced by the extra-individual situation of an individual, by the position he/she has in the group. He/she feels that his/her position in the group does not result from his/her individual efforts. It is mainly the result of how the individuals with whom he/she lives, feel about him/her. He/she may even feel, slightly that besides his social atom there are invisible telestructures influencing his/her position. The fear of expressing the preferential feelings that one person has for the others, is in fact, the fear of the feelings that the others… have for him/her.
… these procedures should be favorably welcomed, since they help in the recognition and in the basic structure of the group. However, this is not the case. They find resistance and even hostility from some people…
Other individuals also expressed fear of the revelations that the sociometric procedure could bring. The fear is more intense in some people and less intense in others. Some may be more anxious to arrange their relationships according to their present wishes, others are afraid of the consequences… These and other facts reveal a fundamental phenomenon, the interpersonal resistance way, resistance against expressing the preferential feelings that some have for the others.
As to the social differences and the injustice regarding the distribution of wealth and qualities, the Morenian concept of Sociodynamic Effect, seems to describe this process. According to him we are different and this differentiation is detected and partially softened by the sociometric procedures. However, it would be utopic to imagine absolutely equalitarian societies (1992: v.3, p. 195).
The hypothesis of the sociodynamic effect states that: a – some individuals from a certain group will be persistently excluded from productive communication and social contact; b – some individuals are constantly neglected, very much below their expectations and others are very much favored, in a disproportional way to their demands; c – conflicts and tensions come up in the groups as the sociodynamic effect grows, in other words, with the growing polarity between the favored and the neglected. As the sociodynamic effect is reduced – reduction of the polarity between favored and neglected – the conflicts and the tensions are reduced.
… However, questions emerged about the possibility of having a society without sociodynamic effect, if such a society has ever existed or if it will exist in the future and if it would be superior to the present one. Many religious societies have tried to eliminate the differential trait from the group, through the suppression of perceptions and differential feelings in their minds, according to their system of values that assume all the men are brothers and sisters and equal, children of god. Therefore, the differentiation becomes a mortal sin and sociometrics, the devil’s science. Another possibility would be to accept the sociodynamic effect as our destiny.
MY OPINION
Envy is a universal human phenomenon, timeless and inevitable. It makes part of the structure of the human psyche and it operates in the human culture and in our social organization.
However, the way of dealing with this feeling varies according to the emotional balance and the self-evaluation that each one of us makes about our qualities, capacities and merits facing the circumstances of life.
In my book, Emotional Survival (Cukier,R.1998), I developed the idea that the different aspects of our identity, or in the terms of Moreno’s role theory, our different relationship possibilities, are organized according to a kind of “System of Self-esteem Maintenance”. I believe that from the first dependency relationships, the central role of our identity is structured. The value the “SELF” acquires at this first evaluation will determine the compensatory maneuvers that it will have to make to maintain its narcissism at tolerable levels.
In the beginning of the intrauterine life, the child does not know where the pleasure and displeasure come from. It experiments psychosomatic roles[39],[ix] as an indiscriminate whole – the child, the world, the mother and the breast, the child the colic, the colic and the mother. Just little by little, as the neurological system matures and though the repetition of the experience, the child begins to associate the pleasure with the presence of the mother or provider and the displeasure with her absence (this referring to a normal child, with normally providing parents).
In other words, what initially was decoded as pleasurable because it satiated a survival physiological necessity begins to acquire certain independence and it does not need the physiological necessity to occur (Freud, 1905:1119-1200). [x] The presence of the mother and/or provider(s) begins to produce, even when there is no necessity to be satisfied. It is the pleasure of being seen touched, looked after, listened by someone who potentially is more powerful and that grants me a certain power if he/she chooses to be with me. The opposite is also true, the experience of displeasure begins to exist each time the provider does not show up, or shows up but does not give all the attention the subject expects.
This new kind of pleasure – displeasure is what will constitute what I call “Narcissistic Economy [xi] or System of Self-Esteem Maintenance”, a second system within the psyche, joined to what regulates the pleasure and displeasure of the body, responsible for determining, all the time, the value of the “self” for the other (how much the other likes the “SELF”) and for himself/herself (self-esteem).
We all know from our own experience that there is a pain that is not physical, but Psychological. The self-esteem needs to be maintained within certain levels of value, otherwise the pain is produced – it is the pain of not being loved, the pain of perceiving yourself of little importance for the other, the pain of feeling vulnerable, the pain of feeling deceived, betrayed, etc. and also the pain of envy, feeling that another one has attributes that you wanted for yourself. This is what Kohut (1984:80-121) calls Narcissistic Injury – the sudden perception that the SELF that thought was valued by the other or by himself/herself, in fact may abruptly lose this power.
The criteria for the SELF to feel valued or not, vary according to parameters stated by the family and socio-cultural environment, from which the subject emerges,they are relative criteria and somewhat flexible, because they change according to the development, the moment in life, etc. However, two rules, extremely simple to be formulated, coordinate the central structure of this value system, one inter-relational and the other one intrapsychic:
1- As inter-relational, I understand all the relationships that one person establishes with other people, since the first relationships with the mother and family members to the most complex adult relationships. This way, every time the SELF feels valued by another, gratuitously or for something he/she has done, his/her intrinsic value and his/her self-esteem heighten; the opposite is also true and the person feels devalued when he/she does not get the attention he/she desires.
2- The intrapsychic one consists of the relationships one person maintains with himself/herself, and in this context the rule for the SELF to know if he/she has or does not have value is even more simple: the SELF likes himself/herself when he/she is liked and he/she cannot tolerate himself/herself if he/she is rejected or despised.
Each person probably has an optimum level of personal value that his/her psyche needs to maintain in order to psychologically survive. When this self-value or self-esteem is very low, defensive resources are created to try to optimize it, through certain strength compensation. The violence originated by the pain of envy would be one of these defensive maneuvers, which tries to compensate for our self-value in the presence of the superiority we perceive in the other.
Therefore, to work therapeutically with Envy, implies reviewing the client’s emotional life and his/her narcissism. It is a task that begins from a present conflict, but goes through the client’s life, making use of dramatic associations and the tracing of repetitions and transferences (Cukier, 1998, p. 69-76). The final objective is to promote repairing in the patient’s Self-esteem Maintaining System, or Narcissistic System that, as I explained before, consists of a kind of self-evaluation central, or in Morenian terms, a permanent socio-auto metric central that we have in our psyche and which informs us all the time which our value is for the other and for ourselves.
HOW DO WE WORK PSYCHODRAMATICALLY WITH ENVY?
In general the theme envy appears indirectly through relational conflicts or, more often, through the client’s observation that the others envy him/her. I have never received a case in which the person identified his/her problem as an excess of envy, for the shame this statement would promote.
For this reason, I think we must work this matter in an indirect way, also following the client’s clues. The psychodrama offers us many resources to advance, from the present scenes of a relational conflict, to the intra-psychic drama, where themes such as self-esteem and narcissism are cleared up. The work with regressive scenes (Cukier, R.-1998:69-76) and their present repercussions is, in my opinion, the most profound in this case.
Maybe what is more difficult, is to begin the warming up for the patient to be willing to approach the theme of the envy. I do this in a subtle way, using the inversion of roles every time the demand comes in the way: “the other envies me”. I ask the patient to be this other one, put yourself in his attitude, experiment life a little as if you were him/her. I explore this inversion deeply, even the feeling of rage that the rival’s attributes cause to the client.
The inversion of roles also allows the client to experiment the theme of the envy from both sides: being the envied and the envious. In both roles we can ask for associations with situations already lived and deepen the psychodynamic.
The interpolation of a sculpture of this conflicting relationship is very useful to work this theme from a distance. I had a client that complained about how much her very rich sister-in-law envied her commitment to work and to struggle for life. In playing the sister-in-law’s role, I asked her to tell me how the wealth could be seen in her way of being, if it was in her clothes, attitude, etc. The client immediately began to describe in details, the clothing brands, her stylists made purses, her shopping at Daslu ( a fashionable Brazilian boutique), etc. Her attitude was majestic, she moved like a queen. I asked her, still in the sister-in-law’s role, to talk about my client, and the first thing she said was: she is poor, she dresses badly, goes shopping on José Paulino (a popular shopping street).
Next, I asked the patient to look at this relationship from a distance and create a clay sculpture of two people who interact like this. What would this sculpture be like? Which attitude would the rich have and which attitude would the poor have? Afterwards, I asked her to name the sculpture. The name she chose was: the slave and the queen.
The theme of the slave and the Queen was the main point of this client’s whole therapy and she gradually faced her feeling of inferiority in childhood. Many scenes were dramatized – scenes at her elementary school, where she always had to borrow the school material because her parents could not afford it; scenes at family meals, where there was not meat for everyone and the parents did not eat it, causing the children to feel guilty – after all, scenes where she learned not to wish what she could not have and to hate people who had them.
Understanding the child’s pain and impotence and learning neither to surrender to them nor making use of the same former defenses, the client was able to perceive that she was an adult; she earned a good salary and could give herself things, objects and things that she would like to have. In the last therapy session, she brought a purse, by a famous brand, saying that it had been a present for herself after having had the courage of looking at her life. We never mentioned the word envy during her therapeutic process and her sister-in-law disappeared gradually from her conflicts.
The technique of the double is inadvisable for the theme of envy. Telling the patient that he/she feels envious is almost like slapping his/her face, the opposite idea from a subtle work.
However, the mirror favors a look from a distance of the conflict, it is a great therapeutical aid. In the case reported above, many insights were obtained when the client, looking from a distance the scene that she had just played with the sister-in-law, remembered another scene, in another context, where she also felt like a slave. The mirror favors the perception of the transferential chain.
Metaphors, maximizations, concretizations, drama games, are all useful and desirable action possibilities especially in group psychodrama, where the theme of envy comes up “in situ”, involving all the participants of the group, even the therapist and the auxiliary ego. There were some group situations that happened often in my clinic, in which a certain client would resent from the attention that I, as a therapist, had given to another client. Mixed with this open jealousy, I have often seen, after some work, feelings of inferiority in relation to the rival, associations to situations of the immediate family, etc, emerge.
The magical store, where the client symbolically buys different kinds of characteristics at the same time he/she sells or exchanges character traits or personality, is usually useful to clarify what is envied in the other.
A very important aspect in therapeutic work with Envy is to help the client go through the mourning of the world’s ideal of justice, to accept the unfair reality of life. Equally important is to accept the feeling of envy, without disqualifying himself/herself, perceiving that it is a human emotion, but that it should neither become an obsession, nor lead to revenging actions, hatred, etc. The client also needs to legitimate the desire that is implicit in the envy and take actions to obtain it. The role-playing technique is very good to learn how to test new roles, attitudes, wishes, etc.
Finally, I should say that an efficient therapy for Envy helps the client to reduce his/her shame, heighten his/her self value, look at his/her own desires and to open to the richness of life. Less physical strength will be used to compare to the others, and more will be used to have compassion for himself/herself and for everyone who struggles to have the best life they can.
CONCLUSIONS
My first intuition in wanting to study human envy would say that this so hidden and shameful feeling was directly or indirectly related to severe psychopathological episodes, such as the psychosis and the borderline episodes.
In fact, a clinical experience of more than 30 years is the basis for this intuition. I have always found, in approaching the intrapsychic of severe episodes, matters related to self-esteem, apparently unapproachable and, many times, the self-deprecation originated from the fact that there had been in the lives of these clients, as well as in the lives of all of us, people with more abilities, more beauty, intelligence, money, etc.
I would ask myself: why most of us are able to deal with these differences between human beings and try to maximize our own attributes, improve our qualities, study, work, progress, while others among us paralyze in face of the same reality, getting obsessed by iniquities, creating supplemental realities to compensate for their lack, developing aggressive mechanisms to “make justice by their own hands” or, desperately have a self-destructive behavior at the impossibility of this undertaking?
Another fact that became evident in my clinic, is that pointing out the client’s feelings of envy, with some exceptions, unleashes negative reactions, sometimes aggressive and of disharmony between therapist and client. In other words, it is impossible to approach envy in a direct and frank way. So, I developed several resources to work with this matter without ever mentioning the word that could come up or not, in the therapeutical process.
However, I remained curious about this great taboo that was so frequent in the clinic. This work has come to satiate this curiosity and provided me with some conclusions:
- Envy is a universal and timeless human phenomenon. It is part of the human psyche and operates in the human culture and in the social organization.
- Opposite to the equivalent feeling of emulation[40], which leads the individual to try to be equal or overcome the other, it paralyzes the one who feels it and makes him/her suffer.
- This suffering is the consequence of the perception of a lack or disadvantage, felt as unfair and demanding impossible repairing actions, unless they are achieve through direct or indirect violence (destroying the rival, social revolutions, boycott, gossip, etc.).
- The pain and the violence resulting from this process are proportional to the dysfunctions in the client’s earlier emotional development. In other words, the less developed and differentiated his/her personality, the more dysfunctional his/her original family had been, the worse his/her self-evaluation, self-esteem, the greater will be the damages in the perception of his/her disadvantage.
- Naming it directly to the client causes shame and maximizes the underlying feelings of inferiority. It is necessary to use an indirect way of working which allows access to a relaxed ground.
Notes
- [ii] For Antonio Damásio a sentiment is a mental representation, a perception of the state of the body, whereas emotion is a reaction to a stimulus and a behavior associated (for example, a facial expression). Therefore, the sentiment is the recognition of an event that is occurring, while emotion is the visible effect of the same. Emotions are corporal things, whereas sentiments are mental things. Emotions are an automatic response. They do not require any thinking. They are the fundamental mechanism for the regulation of life. Emotions precede sentiments, and are the basis for them. I think that envy is a set of sentiment/emotion, that’s why I decided to adopt the term emotional experience in this text, because it is more inclusive.
- [iii] I have chosen to use the term psychosociodrama for I believe that the theme of envy is at the same time collective and individual. Moreno (1975, p. 383-385) says that Psychodrama refers to “private” problems, but as soon as individuals are treated as collective representatives of the roles of the community and of the relations of roles, not taking into account their private roles and their relations of private roles, the psychodrama converts into a “sociopsychodrama” or, more briefly into a sociodrama .
- [iv] Lacan is of the few theorists that sees envy as a triangular relationship. The triad in question would involve the envious, the envied and a “Great other” that would observe and judge them. This theory helps to understand how envy and narcisism are related and that they originate in the phase of psychic development, which Lacan calls the stadium of the mirror.
- [v] For Jung, the Shadow is the Center of the Personal Unconscious the nucleus of the material repressed by the conscience. The Shadow includes those tendencies, desires, memories and experiences that are rejected by the individual as incompatible with the Persona and contrary to social standards and ideals. The Shadow represents what we consider inferior in our personality and also what we neglect and never developed in ourselves. In dreams, the Shadow often appears as an animal, a dwarf, a vagabond or any other figure of lower category.
- [vi] Takahashi and collaborators (2009) in a study about the neurology of emotions used a functional magnetic resonance to examine the activation of the human brain when feeling emotions of envy (pain for the merit of the others) and schadenfreude (schaden = loss; freude = joy, feeling happy with other people’s disgrace). They concluded that when envy was stimulated there was greater brain activation in the anterior cingulated cortex (ACC), region associated with living conflicts, perception of errors, pain through empathy and pain associated with social exclusion. However, in situations that stimulated Schadenfreude, the brain of the subjects showed to be more activated in the ventral striated region, which is connected with reward processes and gratifying stimuli. Thus, the authors interpret that the activation with schadenfreude causes a sensation of pleasure.
- [vii] The neuroscientist Robert Sapolsky in his book “ Monkeyluv: And Other Essays on Our Lives as Animals” , shows that human beings experience abstract feelings with the same neurological system that they use to experience concrete feelings. The pain of social exclusion, for instance, is registered in the brain like any other physical pain.
- [viii] In fact, the matter of envy is mixed with interrogations about merit and justice: the one who has the merits to have the attributes is not necessarily the one who, for right or justice, (changeable according to time in history) has them. The political fights try to change the laws, to minimize the feeling of difference and injustice. Ironically, it will appear again, in the lower level of the new resulting hierarchy, wrapped up in another demagogical ornament.
- Moreno uses the concept of sociometric proletariat to speak about the isolated groups, neglected and rejected, whose feelings do not find reciprocity
- [ix] Says Moreno (1975): “The first roles to appear are the physiological or psychosomatic”. We know that between the sexual role, the role of the individual who sleeps, of the one who dreams and of the one who eats, operational bonds are developed which link these roles and integrate them in a unit. At a certain point we could consider this unit as a kind of physiological self, a “partial” self, a conglomerate of physiological roles.
- [x] Freud (1905) in Three Essays on the Theory of Sexuality, develops the theory that in the origin, the first sexual satisfactions appear by the time of the functioning of the organs that are meant to preserve the life. He speaks about object Anaclitical Choice, showing how the sexual pulsions are based on the self-preserving ones. I think that not only the sexual satisfaction is based on these first experiences of pleasure-displeasure, but also the narcissistic satisfaction of perceiving oneself as target of the attention and value from others.
- [xi] The use of the term “Narcissistic Economy” is analogical, it uses the idea of self-interest (Narcissus who only thinks about himself) but also the idea of hemeostasis or economy, showing the self-protective function of this mechanism in the psyche. The pleasure in this narcissistic system is achieved when the individual’s self-esteem is high and the displeasure or narcissistic pain, when the self-esteem is low.
Bibliographic notes
[1] Aristóteles (1899), Retórica Das Paixões, Martins Editora.
[2] Schoeck, Helmut ( 1987) Envy: A Theory of Social Behavior, Liberty Fund,.
[3] Gonçalo Fernándes De La Mora (1987)- Egalitarian Envy: The Political Foundations of Social Justice, Paragon House Publishers, USA.
[4] Bustos, Dalmiro e colaboradores (1994 )- O psicodrama, Editora Ágora, São Paulo-Brasil, p.362.
[5] Foster, M.G. (1972)-The Anatomy of Envy: a study in Symbolic Behavior, Current Antropology, vol.13, nº2 (April 1972).University of Chicago Press, USA.
[6] Carl Gustav Jung (1991): Fundamentos de psicologia analítica. Petrópolis: Vozes, 1991.
[7] Byington, C.A.B. (2002)- Inveja criativa: o resgate de uma força transformadora da civilização; W11 Editores Ltda. SP Brasil.
[8] Eduardo O. C. Chaves (1991)- “Justiça Social, Igualitarismo e Inveja: A propósito do Livro de Gonçalo Fernandez de La Mora-Revista da Faculdade de Educação da UNICAMP, nº 4, Março.
[9] Siegel, Allen M.(2005)- Heinz Kohut, e a restauração do self- Casa do Psicólogo, pg.184
[10] Shakespeare, W. (1606)- Otelo,Editora: L&Pm, Brasil, 1999 .
[11] Freud, S.(1908)- Teorias sexuales infantis, 0bras Completas, Editorial Biblioteca Nueva, Madrid, España, p. 1262.
[12] Freud, S. ( 1914)- Introducción al Narcisismo, 0bras Completas, Editorial Biblioteca Nueva, Madrid, España, p. 2017.
[13] Freud, S.(1920)- Além do Princípio do Prazer, 0bras Completas, Editorial Biblioteca Nueva, Madrid, Espana, pp.2507.
[14] Klein, Melanie (1974) – Inveja e gratidão: um estudo das fontes inconscientes, Coleção Psicologia Psicanalítica- Imago Editora.
[15] Ulhoa Cintra, E. M.e Figueiredo, L. C. (2004) – Melanie Klein – Estilo e Pensamento, São Paulo, Escuta.
[16] Horney, k.- Feminine Psychology (reprints), Norton, 1922-37 1967. ISBN 0-393-00686-7.
[17] Winnicot D. W. – (1975)- O brincar e a realidade- Imago editora.
[18] Hiles, D.R. (2007) Envy, Jealousy, Greed: A Kleinian approach. Paper presented to CCPE, London.
[19] Suttie, Ian (1935) – As origens do Amor e do Ódio, Editora Ulisséia, Lisboa, Portugal
[20] Bowlby J. (2004) – Perda: Tristeza e Depressão Editora: Martins Fontes, S.Paulo, Brasil.
[21] Hill, S. and Buss D.- The Evolutionary Psychology of envy
[22] Takahashi, H., Kato, M., Matsuura, M., Mobbs, D., Suhara, T., & Okubo, Y. (2009). When Your Gain Is My Pain and Your Pain Is My Gain: Neural Correlates of Envy and Schadenfreude Science, 323 (5916), 937-939 DOI: 10.1126/science.1165604.
[23]Sapolsky Robert M. (2005) – Monkeyluv: And Other Essays on Our Lives as Animals, Scribner, New York, USA, pp. 89-97.
[24] Barrows, K. (2002).- Envy- Icon Books, USA.
[25] Smith ,R. H.(2004) – Envy and Its Transmutations , in A .Tiedens, L.Z. and Leach C.W. ( 2004)- The Social Life of Emotions- Cambridge University Press
[26] Gaiarsa, J. (1978) Tratado Geral Sobre a Fofoca -, Editora: Summus, S.Paulo, Brasil.
[27] Berman Avi ( 2007)- Envy, Competition and Gender: Theory, Clinical Applications and Group Work, Routledge, London.
[28] Gilligan, C.(1982)- Uma voz diferente, Editora: Rosas do Tempos, Brasil.
[29] Chodorow, N (1999) – The Reproduction of Mothering: Psychoanalysis and the Sociology of Gender, University of California Press, U.S.A.
[30] Lerner, H. (1990)- Mulheres em Terapia, Editora Artes Médicas, Porto Alegre, Brasil.
[31] Navarro L. and Schwartzberg S. (2007) – Envy, Competition and Gender, Edited by. London: Routledge.
[32] Rojas-Bermúdez, J. (1998)- De La Invídia y de La Violencia- em Revista da Sociedade Portuguesa de Psicodrama, nº 5, Lisboa, Portugal.
[33] Dundes, Alan (1992) The Evil Eye: A Casebook University of Wisconsin Press, Madison, Wisconsin, originally published in 1981 by Garland Publishing, New York
[34] Franz Anton Mesmer,Origem: Wikipédia, a enciclopédia livre, http://pt.wikipedia.org.
[35] Jean-Martin Charcot-Origem: Wikipédia, a enciclopédia livre, http://pt.wikipedia.org.
[36] Beck, A. T.; Kuyken, W. (2003)- Terapia cognitiva: abordagem revolucionária. In: Abreu c. N.; Roso M.(org.) Psicoterapias cognitiva e construtivista: novas fronteiras da prática clínica. Porto Alegre: Artmed.
[37] Rojas-Bermudez (1997) – De La envidia y de La violencia. Revista de La Asociación Argentina de Psiquiatras, ano 3, v.2, nº 2.
[38] Moreno, J. L.-(1992) Quem sobreviverá? Fundamentos da Sociometria, Psicoterapia de Grupo e Sociodrama, Dimensão Editora, Goiânia.
[39] Moreno, J. L. (1975)- Psicodrama. Editora Cultrix, São Paulo, p. 25 – 26
[40] Houaiss, A- (2001) – Dicionário Houaiss da língua portuguesa, editora Objetiva, Rio de Janeiro.
-
PSYCHODRAMA OF ADDICTION: THE FIGHT BETWEEN THE ADDICTIVE
PERSONALITY AND THE TRUE SELF [1]
I never cease to be surprised when psychodramatically investigating my clients’ addictions. Invariably, the conflict that arises between the drug—the object of the addiction—and the addicted part of the client’s personality is similar to several tragedies described in classical literature. This is the case when referring to Goethe’s version of the Faust myth.
This is the story of the scientist, Faust, who circumvents the laws of the Church in the Middle Ages to search tirelessly and omnipotently for the solution to the mystery of existence. He has knowledge of various sciences, but none of them satisfies his desire to become a kind of “God,” with unlimited access to everything that occurs in nature.
Aware of his human and nonconformist limits, he is approached and seduced by Mephistopheles (the devil). He commits himself to delivering his soul in exchange for knowledge and intense experience of worldly pleasures and in order to have the gift of controlling time and people, causing them to sway according to his wishes.
The result is disastrous. Wherever he goes, Faust spreads unhappiness, and in the end falls victim to his own thirst for omnipotence as he ends up hurting himself and the only woman he truly loves.
Like Faust, the addicted person tries to circumvent the rules of the system. However, in this case, one is trying to circumvent not only an institution, but human nature itself, thereby challenging its essential vulnerability. We humans are powerless when faced with the lack of logic and justice in the distribution of misfortunes and differences¾the family we are born into, health, wealth, beauty, intelligence, etc.¾and faced with a future unknown to us, guaranteeing only our own death, as well as the deaths of those whom we love.
Parodying the Faust tragedy, the true self of a human being sells his soul to the addicted part in exchange for the promise of quick relief of all the sorrows, pain, and frustrations that normal life brings about.
Furthermore, the observation of several clinical cases has made it evident that the potentially addicted person seems to believe that the lives of other human beings are not the same as his own and do not produce the pain and disappointment that he experiences. He therefore feels he is a victim of life, requiring some extra help to finally become “normal.” In fact, he lacks the capacity to elaborate frustrations and grief¾becoming a victim, yes, but of false relief, a victim of the devil-drug that provides a state of temporary well-being and a life sentence.
Why would someone sell his soul to the devil or self-administer drugs that can kill, lead to imprisonment, or jeopardize his health? This is the question that motivated me to study the subject of addictions, about which I will attempt to be as clear as possible over the following pages, as I present the conclusions I reached.
THE HISTORY AND CONCEPT OF ADDICTION (Twerski, 1996)
The systematic treatment of addiction may be associated with the development of the Association of Alcoholics Anonymous (AA) in 1935. This organization arose from the initiative of alcoholism sufferers working together in their efforts to resist alcohol. The symmetry of the participants (there are no doctors, competent speech makers, or health hierarchies) is the main peculiarity of this group. All participants suffer from the same problem. No one is better or worse than any other. This is merely a group of people who support each other and regard each other as equals.
Historically, addiction was thought to be a sign of moral weakness—a practice engaged in by incompetent individuals who cannot deal with reality. Today, we think of it as a physical, emotional, cognitive, and spiritual disease. The research focus on addiction, which was once limited to alcohol and drugs (oral-injectable), has now been expanded to include other compulsive[3] behaviors, such as food addictions, gambling, sex, shopping, work, and petty theft. These behaviors also induce mood swings, social isolation, shame, and despair similar to what is experienced by alcoholics and drug addicts.
Currently, it is understood that all people have the potential to become addicted since addiction is based on the normal desire to go through life with less pain and more pleasure.
OBJECTS OF ADDICTION AND MOOD CHANGES
There are numerous potentially addictive objects: alcohol, cigarettes, food, drugs, gambling, sex, etc. The choice of the object of addiction depends on its availability. It is very common for an addict to replace an addictive object with another; for example, replacing alcohol or cigarettes with food. It is also common for a person to be multi-addicted (Black, 1990: 74).
What all addictive objects have in common is that they produce a quick and pleasant change of mood, which is typically expressed in one of these three directions:
- Excitement – a hypomanic state where the individual feels all-powerful, omnipotent, and complete.
- Satiety – a relaxed state, full of a sense of being, and of anesthetizing against pain and distress.
- Trance – an altered state of consciousness that provides the two previous sensations. It is somewhat hypnotic in nature and creates a rewarding virtual reality where one experiences a state of heightened spiritual awareness.
The seductive and addictive factor of the addictive object rests largely in the fact that it produces these mood changes very quickly. If the effect of the addiction were delayed, the addiction would not occur.
DEVELOPMENT OF ADDICTION
Addiction is a process. It has a definite beginning, though its exact origin is often confusing. It goes through various stages of development and comes to a conclusive end (which sometimes coincides with the death of the individual).
STAGE 1 – INTERNAL CHANGE
Addiction begins when the addict, as well as all normal individuals, experiences a mood change resulting from the object of addiction. The difference is that for him, this quick escape from a painful reality is extremely pleasant and causes an impact of immeasurable intensity. Some gamblers, for example, start to become addicted after the first game in which they won a large amount of money.
From this point, a mental obsession begins to precede and generate the addictive behavior (addictive acting out). In Stage I, the addict behaves within socially acceptable limits. The object of the addiction is like a friend who helps in difficult times—helping the individual to elude and/or cure the pain.
STAGE II – LIFESTYLE CHANGES
Now the addicted person regularly practices his addiction—drinking, eating, buying, consuming pornography, etc. The addictive behavior is ritualized; that is, a sequence of repetitive acts begins to appear. Rituals preserve behaviors and demand that everything be done in the right order; otherwise, they have to start all over again.
The original personality of an individual (the true self) begins to change and accommodate the addicted personality. People who are related to the addict now realize that something is wrong and, simultaneously, he starts to lie to justify or disguise the behavior. The addiction begins to lose its seductive power. It still helps to avoid the originally felt pain, but it also gradually begins to cause some of its own.
STAGE III – TOTAL LOSS OF CONTROL
In this third stage, the addicted side of the personality gains full control over the “true self,” which no longer offers resistance. The well-being once obtained from the object of the addiction succumbs to the stress caused by the accumulated lies, interpersonal relationship tensions, and displeasure at the object’s absence. The addictive acting out starts to bring more pain than pleasure.
The addict is only able to feel peace and security when involved in his addictive rituals. He avoids any close contact that might reveal his total deterioration. On the other hand, he fears being alone, since he is not aware of how to live life itself. He starts to parasitize family members while manipulating them at the same time in order to get them to meet his needs and act as his caregivers. He tends to be viscous, insistent—asking for another chance or playing the victim, while losing jobs, friends, getting in trouble with the law, and reaching overall personal degradation.
TREATMENT FOR ADDICTIONS
Studies of addiction are pessimistic regarding therapeutic successes. The benchmark of 25% of cures is the maximum reported, if all of the following therapeutic strategies are used together: 1) antidepressant medication, 2) attendance at AA meetings, 3) family psychotherapy, and 4) individual psychotherapy. Each intervention removed from this package reduces the chances of success, which is why each will be discussed separately.
1-ANTIDEPRESSANT MEDICATIONSDepression among addicts is difficult to diagnose initially, especially because many patients come to the office in a good mood, complaining of a relational problems, and rarely acknowledging that addiction is their main problem. Instead, the object of the addiction is perceived as a friend who circumstantially helps and can be sent away when no longer needed.
Depression is masked by this self-medication, which makes it difficult to address. Topics such as the injustices of life, gambling, harassment from others, etc., usually occupy the discussions during the first sessions. When the drug problem is addressed and abstinence is initiated, emotional chaos occurs and the frequency of depression increases. It takes much patience on the parts of the addict and his/her family and a great deal of consistency from the therapist.
Studies show that many addicts need to “hit rock bottom”; i.e., an extreme experience of destruction of their own life (loss of employment, marriage, or children, being found drunk in the street, being imprisoned for debts, etc.) before they believe that they have no control over their addiction and start wanting to treat it.
These catastrophic experiences are therapeutic because humans often gravitate from a stressful situation to one that is less stressful. Early abstinence is unnatural because it is less satisfying than the high state that the drug provides. It is like asking someone to throw away their most precious jewel. Only after a person reaches “rock bottom” can this relationship sometimes be reversed and the perception of what is worse changed. The addict becomes frightened by his total decay and wants to do everything within his/her power to once again prevent this catastrophic end.
The crisis (the experience of hitting rock bottom) opens a crack in the delirious protective wall of addictive cognition. It is a rare chance of coming in contact with the real self, but as soon as the crisis passes the crack heals and the delusional system takes over again. Unfortunately, most addicts’ families, wanting to protect their image, cover for the addict, and keep him/her from living out this self-destructive experience. The goal in working with addicts’ families is to help them see that their co-dependence ends up harming more than it helps.
If before abstinence, the patient felt the injustice of his/her reality and the lack of excitement in his/her life, their dissatisfaction following abstinence will take on macroscopic proportions. Many authors indicate antidepressant medication as the first step in treatment, even before abstinence, believing that it will help the addict tolerate the pain of facing reality. Antidepressants are highly recommended, as they are not addictive. Benzodiazepines, on the other hand, should be avoided, since they are addictive, and care must be taken to not replace one addiction with another.
Abstinence is a formidable and very difficult challenge, as it requires
- The addict to lose his/her confidence in his/her ability to control the addiction. He/she needs to know that his/her sense of reality is distorted and he/she cannot rely on him/herself. The extreme experience is a painful fall, but it offers a great lesson. The therapist must help the patient reach the appropriate conclusions.
- Addicts to submit their perceptions to those of someone else in order to see if what they perceive truly exists. Addicts must let someone else (spouse, AA leader, therapist, etc.) take control, and this will be especially difficult for those who were brought up in a dysfunctional environment that led him in the opposite direction.
2) ASSOCIATION OF ALCOHOLICS ANONYMOUS (AA)
Addicts confuse and seduce normal people with their addictive logic. Hence, homogeneous group therapy is especially important, as it requires “a confrontation between equals.” This is the first among the various therapeutic factors described below, and it is largely responsible for AA’s worldwide success. The strengths of AA are as follows:
- It enables the individual to see himself reflected on the members of the group, as in a mirror, and this can be extremely therapeutic because it allows others to point out aspects about the addict to which he cannot admit himself.
- The absence of upper/lower hierarchies and the fact that everyone in the group shares the same addiction and the same shame for intra-family abusive experiences facilitates the approach to the problem itself. “I am one of many, not the weak one in the group.” It also favors the recognition of family values and dispels the myths that stimulate the addiction. For example: a man is only a man if he drinks or having things is having love.
- AA’s twelve-step philosophy posits the spiritual power of a superior, protective, and wise entity (it can be God, nature, health, etc.). This spiritual bias is critical in addressing the “basic insecurity of the addict,” who is naturally suspicious of other humans and of himself. During the first meetings, the attendees must recognize that they do not have control over their disease, but that a higher being does, and that being will help them.
- AA’s notion of time –is to live one day at a time and say things like, “Just for today I will not use the object of my addiction.” This perfectly caters to the enormous difficulty the addict has in delaying gratification. His emotional logic contains only the present—the now! This concept of changing time goes along with the familiar argument: “I can stop whenever I want.” In fact, it is possible. All addicts are experts in stopping a million times, making new resolutions for their lives, and resuming the addiction once again. It is a vicious cycle that can continue for years.
- e) The group supports relapses and welcomes restarts. This can be such a difficult situation to face when one has to overcome an addiction.
- f) Finally, AA assists in the breakdown of addictive rituals and encourages the fact that certain locations should be avoided at certain times; for example, bars, bingo halls, shops, being left alone at night at home[4], etc.
Families of addicts often indirectly stimulate the use of drugs and harbor dysfunctional, co-dependent relational psychodynamics, thus contributing to the addiction by inflicting severe suffering on the individual. Drug use may, for example, be encouraged by family habits that are apparently trivial at first glance, such as excessive use of self-medication, social drinking, smoking, use of caffeine as a stimulant, using food for emotional gratification and comfort, overworking, etc. Children and young people grow up watching adults seek relief from their conflicts and pain with these practices, and this can create future models of conduct in which the children seek to engage.
Moreover, being with addicted individuals can be quite destructive to one’s psyche and the added contact may demand the addition of specific support measures. AA includes groups that support the family members of alcoholics and addicts. These are Al-Anon (for family members and friends of alcoholics) and Nar-Anon (groups for addicted people’s families in Brazil). In these groups, you learn to deal with the psychodynamics of co-dependency. Their fundamental teachings are:
- No one is responsible for the disease of another person, nor for his recovery.
- One should not suffer because of someone else’s actions and reactions.
- One should not allow oneself to be used or abused in the interests of another person’s recovery.
- One should not do for others what they should do for themselves.
- One should not manipulate situations so that others eat, sleep, get up, pay the bills, or do not drink.
- One should not cover up the mistakes or carelessness of another person.
- One should not create a crisis.
- One should not prevent a crisis, if the latter is in the natural course of events.
Families are monitored to detect the presence of a certain emotional detachment in order to protect themselves and allow the addict to try to “hit rock bottom,” the extreme experience that can possibly help overcome the addiction. Topics such as loyalty, shame, guilt, and secrets, are shared within the groups, and the results are normally very good.
4) INDIVIDUAL PSYCHOTHERAPY
It is not easy to therapeutically approach people because of the impenetrability of this mindset dominated by a logical and biased way of thinking and because of the changes in the conception of time.
What we have achieved, in general, is an apparent improvement at first, followed by a relapse and abandonment of the therapy. I worked once with an obese man who lost 70 pounds in three years of individual psychotherapy, only to recover them all back in two months and leave the treatment at the end. Preventing relapses must be a constant concern from the very beginning of therapy.
I think the psychotherapist who cares for addicted people needs to be humble enough to admit that he cannot deal with the problem alone. The pleasure that the drug provides is much more enticing than one hour per week of reflective work. The advice of a psychiatrist and the inclusion of AA are necessary, at least at some point, for both the patient and his family to successfully complete therapy.
One should also avoid, at all costs, the seductive role of “savior of the world,” and should not be the controller of drug intake, diet, expenses, etc. to prevent being taken in by the codependent psychodynamics and losing one’s operability. These are issues and practices that can be discussed in psychotherapy, but it is not the therapist’s function to control them.
Winning the trust of the addict is the first step, and he should be warned that he would feel a great deal of discomfort during psychotherapy. In addition, he should be made aware that he may have to be medicated and, that he may at some point need to attend AA. If the patient does not agree to these conditions, it is preferable to not accept him into psychotherapy and to keep “the only remaining bullet” for another time when he really wants to be treated.
THE PSYCHODYNAMICS OF ADDICTIONS – “THE TRUE SELF (“I”) VS. THE ADDICTED SELF (THE ADDICTED SIDE OF THE PERSONALITY)
In working with addicts during psychotherapy, the therapist must understand that two client personalities are present at all times: one that wants to collaborate (“I”) and another that surreptitiously seeks to boycott, lie, and end any effort to push him away from drugs (the addicted side).
The addiction process either starts randomly or as a result of some discomfort. The object or addictive practice creates a sense of well-being or perfection—at least for a while. The “I” feels guilty and anxious. These are initial warning signs that, unfortunately, fail to inspire action over time.
Each time the addiction acts, the addicted personality gains a little more control. The “I” disapproves of this way of acting, feeling and thinking, but it loves the mood change that the addictive object provides. It promises to control the addict with its willpower and sometimes succeeds, but it eventually succumbs to the addicted personality. The “I” gradually becomes less tolerant of the discomfort, and any frustration is experienced as pain, thus signaling the need to seek out the object of the addiction.
Addiction is the denial of emotional pain and a refusal to depend on the help of other human beings for relief. The addict does not care for his wife or children, or even for himself. He ignores the fact that he can get sick or even die. The addicted self dreams of escaping pain, obtaining peace, sensory perfection, and immediate gratification, while the “I” dreams of controlling the addict through the addict eventually losing energy, giving up, and surrendering.
It is a vicious cycle. The more the “I” seeks relief in the addiction, the more shame and guilt he feels and the more he undervalues himself, which increases his pain and initial discomfort. Then, once again, he seeks relief in his addictive practices, and the cycle resumes. Figure 1 illustrates this process:
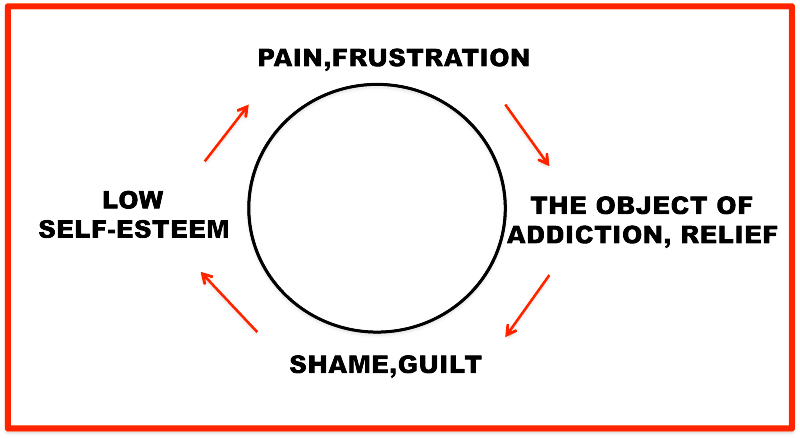
FIG 1-THE VICIOUS CYCLE OF ADDICTION
For psychotherapy to be effective, the patient has to understand this cycle and realize that he has no control over the addiction. The addicted side is much stronger and articulated, and even in abstention will prove a threat to the self.
PSYCHODRAMA AND ADDICTIONS
Studies of traumatized animals and patients (Mary, 2004; Van der Kolk, McFarlane & Weisaeth, 1996) suggest that experiential psychotherapies are more effective than just verbal therapies.
The immediate response to a stressful situation[5] triggers reaction mechanisms of the sympathetic nervous system, known as an “alert reaction.”
The animal’s body prepares for either fight or flight (Cannon, 1939; MacLean, 1952). When it is prevented from reacting, the animal’s brain works through archaic mechanisms (Levine, 1999), causing the “freezing” of vital functions. This device allows the animal, pretending to be dead, to fool its predator into leaving it alone, or at least to gain some times in coming up with another escape strategy.
Apart from a few differences, the same thing occurs with humans. When we are unable to respond, our brain works with its reptilian layer, and the freezing of vital functions manifests itself through shallow breathing and hardened muscles, simulating rigor mortis. Additionally, the individual’s mind is numbed mind, resembling a zombielike state.
However, unlike an animal, the human being doesn’t “thaws” once the danger has subsided by exhibiting observable bodily tremors. Human beings tend to intermediate these physical functions with thoughts, feelings, emotions, and invisible allegiances, which are the products of the two remaining cerebral layers. What remains missing is a combat action, the resumption of control, which is sometimes only achieved many years later, due to the active repetition of violence or abuse, as a way of sometimes clumsily mimicking the abuser, or the one who has control.
Dramatization provides the opportunity for this missing action to occur, thus allowing the muscles a safe discharge from the body’s need for resumed control. It should be noted that psychodrama was one of the first body therapies to be used, and Moreno has already pointed out that the body remembers what the mind forgets, especially events that take place in early childhood—even before the emergence of language. The best way to recapture the memory of actions is through expressive methods that involve the whole person (body and mind) in the action. The following is a description, illustrated with by real case studies[6], how I use psychodrama to help with this type of problem.
IN INTERVIEWS
Clients who come to us do not know what psychodrama is, and many do not even know what psychotherapy is. It is quite likely that the vast majority of laypeople think that they should just spend some time with us and tell us about their lives so we can provide them with solutions to their most intimate problems. In addition, some clients are afraid of our profession because we are either seen as wizards who can read souls, or as arrogant people who feel superior to others.
I believe we need to help our patients know who we are, build their confidence in what we do, and help them to become familiar with our working tools. Trust and knowledge are constructed gradually, which is why I perform at least three interviews before accepting a client into a psychotherapy contract. I conduct one or two verbal interviews, a social atom that introduces psychodrama to the patient, and a feedback interview where I summarize my opinion and establish the contract regarding what will be worked on. I specifically perform with the addicted patient, when possible, three different social atoms in addition to the verbal interviews: a traditional social atom; a social atom that occurs during the addiction (Figure 2); and a family atom, or genogram, of the addictions (Figure 3).
1-TRADITIONAL SOCIAL ATOM
Objectives: To explore the sociometric context in which the patient is inserted and to train them for future dramas. It is important to discover their natural auxiliary egos; i.e., understand those who can support the client in the case of depression. In addition, it is helpful to identify which sociometric spaces are missing from his social atom. Sometimes we see an adult surrounded by his/her primary family members but has no friends, as if he/she were a child in the care of his/her family. Drawing the client’s social atoms at the beginning and end of the therapeutic process, according to protocol, and comparing these images can be very useful in assessing the effectiveness of the therapy.
2-THE SOCIAL ATOM DURING ADDICTION
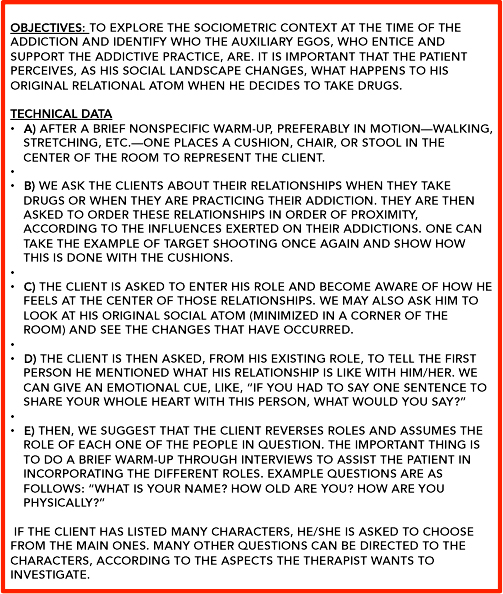 FIG 2-THE SOCIAL ATOM DURING ADDICTION
FIG 2-THE SOCIAL ATOM DURING ADDICTION3- GENOGRAM OF THE ADDICTIONS
Objective: To investigate the presence of addictive habits, compulsive and/or abusive, which act as shame generators in the client’s family atom.
Technical data: The client is asked to rate, on a scale from 1 to 10, the presence of the following behaviors evidenced by some member of his/her family: addictions (drink, drugs, shopping, food, work, etc.); perfectionism; procrastination[7]; anger; victimization; depression; compulsion; suicide; or any other dysfunctional habit.
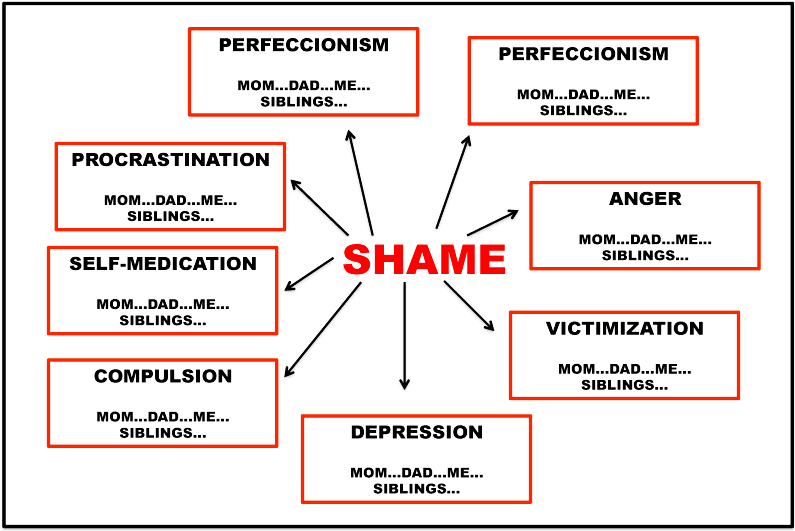
FIG. 3 – GENOGRAM OF THE ADDICTIONS
Both the social atom during the addiction, as well as the genogram of addictions, help the therapist and client to focus on the extent of damage and family influence. They also help to prevent a relapse, as they materialize, in an obvious manner, people and situations the addict must avoid if he/she does not want a relapse.
AT THE BEGINNING OF THERAPY – SPECIFYING THE TRUE SELF OF THE ADDICT
- USING MASKS
V., 35 years old, unmarried and obese, with two children, owns a company that is facing serious administrative problems. She complains about nocturnal bulimia,[8] which she cannot control. On these occasions, she devours everything that appears in front of her, whether savory, sweet, fruity, ice-cream, etc.
“These are moments of gastronomic madness,” she says. “I put on all the weight I lost previously with diet and exercise.”
In the first few sessions, she said she wanted to work on[9] the “crazy fat person that appears at dawn.” I asked her to imagine the scene in which this “crazy fat person” last appeared. She set up the scene in her home kitchen the night before. She was alone, looking inside the fridge and in the cupboard for anything she could eat.
We set up this kitchen space in detail, and before we started the scene, I asked her to begin her soliloquy one minute before she went to the kitchen:
- (in soliloquy[10], one minute before): I’m sad, alone, and afraid of what will happen tomorrow (referring to a serious problem in the company).
T.: Okay. Now, continue the soliloquy, but go to the kitchen until the “crazy fat person” appears.
- (in soliloquy): I want to sleep, switch off, and not think about tomorrow. At this moment, she stops and says to T.: The “crazy fat person” begins to open the refrigerator.
T.: Very good! Freeze a little and choose a mask with which to be this “crazy fat person.”
- goes to the wall where the masks are hanging and carefully takes down a chubby face with red cheeks and a feather on top of the head and says: This is the one, without a doubt!
T.: Wear it for a while and imagine this scene: V. is alone, worried, and sad. She goes to the refrigerator (T puts down a cushion to mark the role of the client), and then you show up, enter the scene, and talk with V.
- (with the mask, in the role of crazy fat person): I came to help you, dear (in an exaggerated way). I’m your dear friend. I always fill you up with something and make you sleep. Come, and I’ll sing you a lullaby.
T.: Change places for a while. Take off the mask (T. puts the mask on the pillow, and V. assumes her proper place at the refrigerator door).
- (as V., towards the “crazy fat person”): Get away from me. You don’t help me. I need to lose weight to change my life, and you don’t let me. I’m still fat and alone. Go away. I hate you!
After a few more role reversals[11] to deepen the characteristics of V.’s split aspects, T. asks V. to leave the scene and watch while he sets two pillows—one with the mask and one without—and quickly repeats the dialogue quickly (so that the client does not get “cold”).
Then, he says: “These two parts are yours, V. One brings you to therapy, and the other offers you the addiction. We need to know them better, and we will do so from now on.”
- EXECUTING DOUBLES[12] OF THE ADDICTED SIDE
It is very useful to run doubles of the addicted side, especially emphasizing the paradoxical nature of this side of the personality.
Crazy fat person: Bring me your pain, and I’ll give you relief.
T., as a double (of V., in the role of the crazy fat person): Bring me your pain, and I will give you the illusion of relief.
Crazy fat person: I shall set you free.
T., as a double (of V., in the role of the crazy fat person): I will be your only boss.
Crazy fat person: Spend some time with me. You can trust me. You can trust no one else.
T., as double (of V., in the role of the crazy fat person): Spend some time with me, and I’ll teach you not to trust anyone.
Crazy fat person: I’ll teach you a way to not face your problems.
T., as double (of V., in the role of the crazy fat person): You will get rid of the problems for a short time, but they will not go away.
Over time, T. may propose that the client takes on the double role of the addicted side herself, in order to internalize a type of reasoning that is less influenced by the addicted logic.
C) WRITING LETTERSWriting letters is a good way of discriminating parts—those of the writer and the reader. It is my favorite strategic resource for maintaining the link between sessions. In the case of addiction, we suggest that the letters be written in several directions:
- From the addicted side to the self
- From the self to the addicted side
- From the body to the addicted side
- From the object of addiction to the self
- From various members of the social atom to the self
- From the addicted side to the most intimate family relationships, etc.
- D) BUILDING METAPHORS FOR THE ADDICTED PART
W., a 42-year-old, highly successful homosexual professional, has a partner with whom he has lived for 20 years. He’s a “sex addict,” with possible compulsions to leave at daybreak and have sexual intercourse with strangers without using protective measures.
“Like a vampire hunting for blood,” he says spontaneously, referring to this ego-dystonic part of his personality. I asked him to forget himself and to play the vampire role and to tell me his story, with a beginning, middle, and an end.
“I was a handsome young man,” he says, “when one night, walking casually down the street, I was attacked and bitten by a vampire. I lost the freedom to be who I wanted to be, and I transformed into a vampire. Being a vampire is not a choice. It is my destiny.”
I asked him to show, with his body, how he felt as a vampire. He folds into himself and says, “Ashamed.”
I get closer, put my hand on his back, and ask him, “When, before, have you felt so ashamed?”
“When my father beat me in front of everybody,” he says, referring to a scene that occurred when he was five years old. Often, throughout his psychotherapy, we worked on this scene to understand the vampire side of his personality.
As you can see, metaphors are great resources with which to bring out split worlds—parts not assumed of the life story and of the clients’ selves. They allow multiple therapeutic uses and can be brought forward spontaneously, as in the cited example, or built through the implementation of some behaviors, feelings, etc.
E) THE EMPTY CHAIRThe therapist places an empty chair in front of the client and urges him to imagine there are people sitting there, or parts of himself with whom he wishes to work. In the case of the addiction, the drug itself can be embodied there, as well as the partners of the addiction—the addicted side of the personality that dominates the self, metaphors, dreams, etc.
The role-playing is done with the client changing positions; i.e., the client plays a role, then he changes chairs with another person, and the other person starts role-playing. This is role-playing without dramatic action. This technique can be used as an initial warm-up, followed by open stage work, or as a single technique within a psychodramatic work.
I like to ask the client to talk to the drug, reverse the roles and, after some time, he/she becomes the double of this object or addictive practice in order to externalize the unsaid—the future consequence—and to finally be able to appropriate itself and not dissociate from the full experience. The therapist may play roles as well, if he wishes, or he can merely observe, interviewing both conflicting parties and presenting a point of view that was not addressed in the dialogue.
- (40 years old; smokes marijuana all day in the car, at work, at school, etc.) to the empty chair, where marijuana sits: I need you.
C., as marijuana to C.: Me too. We are an inseparable pair.
C., to marijuana: But I’m missing classes and may lose my job.
C., as marijuana to C.: Well, that’s what they say. We understand things better—more deeply.
C., to marijuana: No way. I do not even remember what I have to write today. I have to ask Luis.
C., as marijuana to C.: That idiot, C.D.F…
- asks C. to get up, places a cushion in place of C., and says, “Now I’ll be marijuana and you stay behind me, explaining what I—marijuana—am not saying.”
T., as marijuana to cushion representing C.: Luis is an idiot. He has a stupid face. He knows nothing.
C., as marijuana twofold: Stay only with me. I’m your only friend. Don’t study. Don’t date. Only with me will you be happy.
C., as C. to T.: It is just like my mom, who does not like any girlfriend of mine. It seems to want hold on to me.
- then asks C. to construct a recent scene in which his mother displayed this domineering aspect, and the session continues with a classic psychodrama, using typical psychodrama techniques.
In fact, there are many ways to promote the discrimination of these parties that are in conflict, and I find it extremely useful to spend some time of the therapy session processing this division.
ENTERING INTO THE PSYCHODYNAMICS OF THE CLIENT – WORKING WITH THE REGRESSIVE SCENE (Cukier, 1998: 67)
The intrapsychic psychodrama (Pitzele, 1992) with regressive or infantile scenes is a powerful resource for working with addictions. Its basic goal is to reframe issues related to self-esteem, discriminate infant pain defenses, and evaluate the function of current addictive behaviors within the context of the client’s life story.
In my book, Emotional Survival, I describe in detail the management of drama with regressive scenes. Figure 4 schematically shows the steps that need to be covered in this paper, and Figure 5 provides a roadmap to interviewing the client in his role as a child.
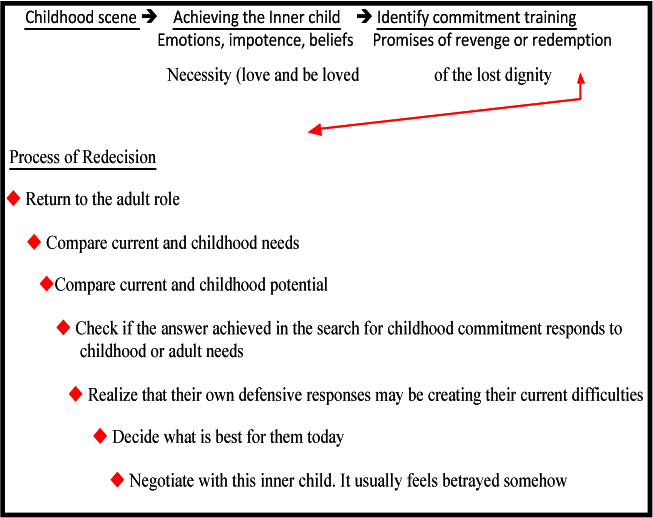 FIG. 4- WORK SCHEME WITH CHILDHOOD SCENE
FIG. 4- WORK SCHEME WITH CHILDHOOD SCENE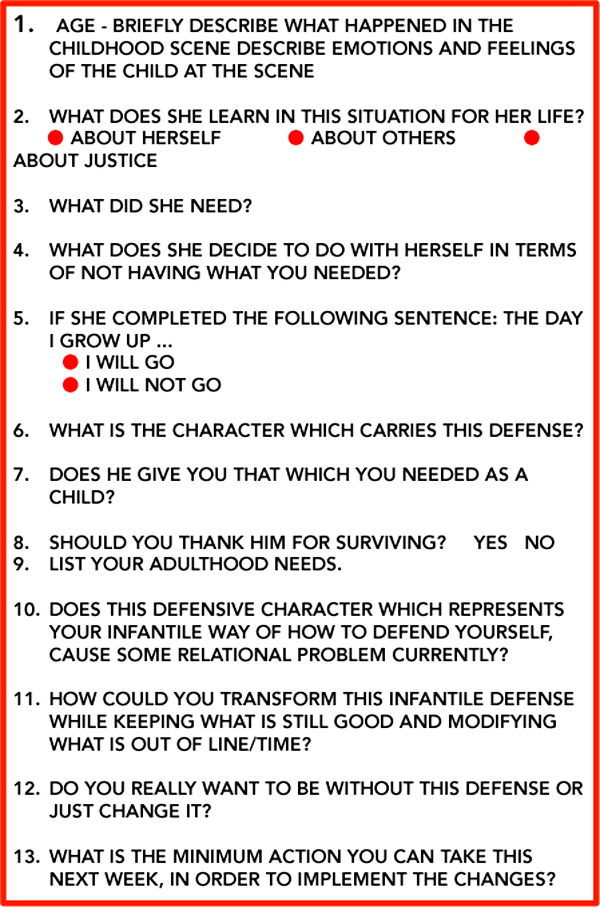
FIG. 5 – SCHEME OF INTERVIEW WITH THE CLIENT IN THEIR ROLE AS A CHILD
Many sessions take place in order to process the material obtained in a traumatic childhood scene. We seek the communication of the adult part of the personality with the child part in order to make a sort of negotiation and “redecision.” The client’s adult part needs to understand this inner child’s concrete thinking and negotiate with it in order to obtain alternatives that do not compromise health and happiness.
A drama with the regressive scene runs out only when the client:
- Relives the pain of the childhood scene
- Gains the ability to understand what he did to survive
- Understands the current problems caused by his childhood defenses
- Exercises new forms of appropriate adult actions by modifying his current conduct
It is evident that a session of only 50-60 minutes cannot account for all these aspects. I have worked for about three months on a scene to understand the most part of the connections. This work represents the center of the hurricane. It is the most important bullet shot with our trigger, and we should not spend it in vain by going too fast.
There are many ways to finish a session in the middle of this work, leaving some links open in order to reignite the patient’s and continue the following week. With this aim in mind, certain strategic tasks, like homework, are given. These include:
- Write in detail and bring in for the next session what happened in this scene. If you have a picture from that time, bring it as well.
- Write a letter to yourself as a child. Take care to write in child language, because the person who will read it is a child under eight years of age.
- Make a collage or find a picture on the Internet of the character that carries your childhood protection.
- Take a picture of this scene in an imaginary Polaroid and continue with it next week.
- Write a letter to each of the characters in this scene (father, mother, brother, etc.) What would you say to them today about what happened in that childhood scene?
- Imagine if the world’s best lawyer could defend this child. What would his argument be?
- What would the child who you once were ask you for, if he could?
Sometimes the client does not want to continue the work the following week because they have something more urgent to work on or because they do not feel prepared to enter into the old anguish. The task is then deferred to when he can resume it. Sometimes the client does not complete the task. He forgets about it or does not want to do it alone. We can help the client implement the work during the next session or let him bring it for the next time. It is always good to discuss why the task was not done because it is representative of an agreement with the therapist that was signed and broken.
Let me describe an example where I used this technique with a shopping addict client:
A., a 35-year-old compulsive shopper spends money he does not have, buying things he often does not use. In a particular session, he says he wants to work on the “urge to go to a certain store in São Paulo, known for its sophisticated, international, and extremely expensive products.”
- to A.: Go around the room, stretch your body, and start thinking of when you felt this urge most recently.
A.: Yesterday, after walking in the morning.
T.: Where were you?
A.: When the urge started?
T.: Yes.
A.: I was combing my hair after my bath.
T.: We will set up your bathroom—the mirror … Where is the door of this room?[13]
- Patiently provides the locations of all the bathroom parts—the cabinet, mirror, etc.
T.: Begin to comb, and start a soliloquy.
A .: Today I am well. I should fit into those leather pants … I need to buy them. If I go to the store, I can pay in ten installments. I can even wear them tonight to C’s party.
T.: Take a deep breath, close your eyes, and enter yourself. Look for what you feel in your body when you start to think about it.
A.: My hands shake and sweat. I get excited
T.: Let this excitement take care of your whole body. Starts jumping higher and higher. He laughs.
T.: Very good. Higher. Jump higher … What does this joy remind you of?
- (Immediately): My father coming for me every two weeks. I was waiting at the door. We were going to the restaurant, bowling, or shopping. He bought everything I wanted. He had more money than my mother. My mother even told me to ask him for things.
T.: One day in particular?
A.: Many similar days. I had a father every two weeks.
T.: We will set up one of those days here … Remember a moment from one of those days.
A.: Buying a car game ( an expensive motor car race) . It was a big toy store there at the top of Lapa (it is a district in S.Paulo)… We had already gone there on another week … We went in the morning—on Saturday. Then, we set it up at his house. We set it up all afternoon. He and I were very happy.
T.: A., take a deep breath and close your eyes. Picture this scene inside you, and especially look at your face, your body, and your age. What are your emotions right now?
A.: Joy. Joy!
T.: What did you need at this point in your life?
A.: I needed this time not to end and for it not to be so rare (he cries) … He died when I was 12, and the two weeks were over.
T .: Take a deep breath and go back to the scene within you … What are you learning at this time in your life that you will never forget?
A.: I like my father, even though my mother did not (crying). He is good to me. He likes playing with me (more crying).
- (Going to the corner where he minimized the bathroom scene and the shopping urge): Look at this 35-year-old man here … He needs to go to this store to buy this expensive object … Do you have something to talk to him about—your nine-year-old self—this very minute?
A.: Your father is not there, you idiot (crying) … You will only get in trouble.
T .: Go back to your adult role, A. In front of the mirror … Look for a minute at this boy (points to the childhood scene in which the cushions mark the roles) … Do you think you could get in touch with him during the week—write him a short letter? I feel that you need to talk. It seems that there is some relationship between your father and the car game , the urge, the leather pants, and the chic shop … Think about it, and we will continue in the next session.
In the next session, warmed up by the note that the client, in his adult role, wrote to his boy self, we resume his father’s death scene. The patient, age 12, is in front of his father’s coffin, sad and angry, because his mother and the new father’s wife have created a tense atmosphere at the funeral.
T., for A.: What do you need at this point in your life?
A.: For my mother to stop thinking only about herself and think of me and keep me.
T.: What do you learn by not having what you needed?
A.: I have to be on my own from now. Nobody will care for me.
T.: What does this mean for a 12-year-old boy?
A.: That I have to look for a way to make money so I get all I want.
A., to T. (out of the child role and speaking as an adult): Buying all I want is a way to do this, isn’t it?
T.: It seems so. Buying all you want is to have a father within, and this is what we need to change.
4- End of psychotherapy – setting new behaviors and new sociometry
The addictive behavior is a safe behavioral and predictable mode of preservation, but it is dysfunctional and uncreative. Psychodrama can do much to develop the spontaneity of the patient to help him train new behaviors and build risk in new sociometries.
Techniques such as role-playing, dramatization of feared scenes, and dramatic games help to reveal fears an individual might not otherwise be aware of, behaviors not developed, and roles not played. I like setting up my office as a privileged and magical laboratory, where pigeons and colorful scarves come out of a black top hat and are later transformed into new dreams, future projects, and new relationships.
FINAL WORD – RELAPSES
Relapses in addiction are normal. The therapist should inform the client that he is already expecting this and that he will certainly never stop helping him. There is a tendency, almost generalized, for patients to end the therapeutic process following relapse. This is because in addition to being disappointed with the therapy, their self-esteem is very low. They have catastrophic thoughts of personal ruin, which in turn lead back to the cycle of the addiction.
Therapists need to pay attention to relapse situations because they are often repeated and because we can predict them if we watch for some indicators. These are some signs the client may show of a possible relapse: skipping therapy, showing remorse and shame, starting to blame others for their problems, self-victimizing, staying slow and repetitive, etc.
Those who relapse do not restart from zero, because they have already made some progress and need only to resume control. Making a prognosis of relapses early in the treatment and paying attention to life situations that may encourage them can shorten the resumption of control process.
Returning to AA is also very difficult the second time, especially for the group shame it brings and because it discredits the therapeutic capacity of the meetings. Individual therapy needs to focus on improving this process of resuming group meetings.
It is desirable for the therapist to share his own mistakes because it can act as a model for the patient. “If my doctor or therapist makes mistakes, apologizes and starts all over again, I can too.” Errors do not demolish a person. The best thing is to admit them promptly and fix them as soon as possible so that the denials and lies do not accumulate.
RECOVERY
To recover from an addiction is to break the dependence of the internal addictive ritual and discover a new way of living—one that is more vulnerable to fears, conflicts, and relationships.
Changing the self-image is one of the most difficult aspects of the therapeutic process, and the shame for actions committed in the past can ruin recovery. The therapist must help the client transform shame into guilt, which will naturally generate remedial action.
Learning to admit mistakes is one of the goals of therapy. I often reframe what clients mean by human nature telling them that to be “human” is to make mistakes and to seek to get it right the next time. Moreover, our admitted vulnerability generates a secondary benefit, which is to encourage empathy from other people and bring them closer to us.
Omnipotent people who know everything and do not need help from anyone else, in general, are lonely. We connect with other humans through our very human faults.
REFERENCES
- Black, Claudia (1990). Double duty – Food addicted. Denver, Mac Publishing.
- Bradshaw, John (1977). Curando a vergonha que me impede de viver. Rio de Janeiro,
- Record/Rosa dos Tempos.
- Bustos, M. D. (1990). Perigo, amor à vista. São Paulo, Editora Aleph.
- Bustos, M. D. (1992). “Novos rumos em psicodrama”, São Paulo, Editora Ática.
- Bustos, M. D. (1994). “Wings and roots”. In: Holmes, Paul; Karp, Marcia & Watson, Michael.
- Psycodrama since Moreno. No Brasil, publicada por Leituras 2 – Companhia do Teatro Espontâneo.
- Cannon Walter (1939) – The Wisdom of the Body, Nova York, Norton, Citado por Anne Ancelin Schutzenberger – “ Querer Sarar”, Editora Vozes, Rio de Janeiro, 1995.
- Cukier, Rosa (1998) Sobrevivência emocional – As feridas da infância revividas no drama adulto. São Paulo, Ágora.
- Dayton, Tian (2000). Trauma and addiction – Ending the cycle of pain through emotional literacy. Florida, Health Communications, Inc..
- Ericson, E. (1976). Infância e sociedade. Rio de Janeiro, Zahar Editores.
- Frankl, Viktor Emil (1998). Em busca de sentido: Um psicólogo no campo de concentração. 8a. ed. Rio de Janeiro, Vozes/Sinodal.
- Le Doux, Joseph (1996). O cérebro emocional. Rio de Janeiro, Objetiva.
- Levine P. A. (1999) – O Despertar do Tigre, Curando o Trauma – Editora Summus, S.Paulo.
- MacLean D. Paul (1973)- A Triune Concept of the Brain and Behaviour ,University of Toronto Press, Canada.
- Mary W.S. (2004). The limits to talk – Psychotherapy Networker January/February.
- Mellan, O. (1995). Overcoming overspending. Nova York, Walker and Company.
- Perazzo, S. (1994). Ainda e sempre psicodrama. São Paulo, Ágora.
- Pitzele, P. (1992). “Adolescentes vistos pelo avesso: psicodrama intrapsíquico”. In: Karp, Marcia & Holmes, Paul. Psicodrama – Inspiração e técnica. São Paulo, Ágora.
- Twersti, J. A. & Nakken, C. (1999). Addictive thinking and the addictive personality. Nova York, M.JF Books.
- Van der Kolk, B.; Mc.Farlane, A.; Weisaeth. L. (1996).Traumatic stress: the effects of overwhelming experience on mind body and society. . Nova York, Guilford Press.
- [1] This article is mainly based upon the book “The addictive Personality”(1996) from Twerski, J. A, that I deeply recommend readers to read.
- [2]. Psychologist, Psychotherapist, Psychodramatist ,by S O P S P (Psychodrama Society of S. Paulo) and by Jacob Levy Moreno Institute of São Paulo.
- [3] Obsessions and compulsions are related and, in general, accompany each other. Both involve people becoming consumed by something irrational. An obsession refers to an irrational idea and compulsion (an irrational act). Obsessions and compulsions are like post-hypnotic suggestions. There is an irresistible urge attached to them. Some authors argue that compulsive behaviors are actions whose sole purpose is to keep the individual busy so they do not experience feelings of anxiety, boredom, depression, and anguish. They become occupied with something beyond themselves in order to flee from their troubles.
- [4] Most obese individuals, bulimics, and people who eat compulsively eat at night and hide themselves away from everyone else’s sight.
- [5] A stressful situation refers to any situation that leads the individual to a state of despair, either due to a battle to preserve his own life or the life of someone who is important to him.
- [6] All patient names are fictitious, and the client descriptions themselves are mixtures of many cases. I will use T. and the initial letter of the client’s fictitious name to differentiate between the therapist and the client in the cited examples.
- [7] Procrastination: the habit of leaving tasks that should be done now till later
- [8]Bulimia nervosa is essentially characterized by the presentation of binge eating and inappropriate compensatory methods to prevent weight gain (purging, fasting, or exaggerated exercise). Furthermore, the self-assessment of individuals with bulimia nervosa is excessively influenced by body shape and weight.
- [9] I always ask at the beginning of the sessions what the patients want to work on in that session. I believe this simple question encourages client autonomy and responsibility during the time we spend together.
- [10] Soliloquy = this psychodramatic technique consists of asking the client to “think out loud”, as if there were a loudspeaker in his head.
- [11] Role Reversal = in this technique the therapist ask the client to take the other’s place, playing the role of somebody whom he has been talking about – rather than just talking about this person. Using the interview technique the therapist helps the client to compose this character and empathize, little by little, with its perceptions, emotions, and opinions.
- [12] The double’s aim is to get in touch with the client’s non-verbalized, sometimes even unconscious, emotions in order to help him express them. The more the therapist is identified with the client, the better double he will be able to play. I normally say to the client that, for a brief moment, I will stop being me and I will take his place. Through short but precise talks, I try to show him what I have observed. Finally, I let him know I am back to my role as director.
- [13] I always start the scene setup by the entrance door of the place where it occurred. It helps me define the space and warms the client up because he realizes I really know where the furniture, window, etc. are.
ARTICLES
Articles summarizes some of the professional concerns of the psychologist Rosa Cukier. She was always interested in issues related to child abuse, narcissistic and borderline personality disorders and how these issues influence the personal and professional life in adulthood.
Humans exert enormous power over each other, the power of life or death. From a physiological point of view, humans reproduce very similarly to all mammals and are born when they leave the womb.
From a psychological point of view, however, their reproduction is totally unique and peculiar. Psychologically human beings are born slowly and not always completely, depending on your personal determination and luck to find parents who can manage their basic needs.
The human child has two kinds of needs:
– PHYSICAL – a human baby is born extremely fragile requiring physical care (feeding, hygiene, health, heat, tactile stimulation, etc.) without which he dies. The focus here is on what is done to the child.
-EMOCIONAL – Basic emotional need of the human being and without which it does not survive psychologically is the need for dependence, to count on each other. The human baby is born completely unprepared and will only be autonomous, with internal resources, after many years (in the middle class in our urban culture, only after adolescence). Here what matters is not having physical needs met, but how it is done.In addition, the first stage of our life is pre-verbal and everything that happens to us depends on the verbal and emotional decoding of our mother / caregiver) . Without someone who can mirror our needs and emotions we have no way of knowing who we are. On the other hand how this person decodes our messages ends up constituting what we are, and it does so according to their own heritage of emotional experiences.
This first caregiver or caregivers work as a kind of relational bridge between the child and the world and take up, at first the place the “I” * child will take later. We are “WE” before being “I”, that is, the relationship we establish with our first caregivers, is the foundation stone of our identity (Erikson, E,:. 1976) and will also reflect our expectations of the world.
Abused children in these basic and fundamental care are like ticking time bomb for the future. The abuse reverberates throughout his personal and professional life.
Articles summarizes some of the professional concerns of the psychologist Rosa Cukier. She was always interested in issues related to child abuse, narcissistic and borderline personality disorders and how these issues influence the personal and professional life in adulthood.
Humans exert enormous power over each other, the power of life or death. From a physiological point of view, humans reproduce very similarly to all mammals and are born when they leave the womb.
From a psychological point of view, however, their reproduction is totally unique and peculiar. Psychologically human beings are born slowly and not always completely, depending on your personal determination and luck to find parents who can manage their basic needs.
The human child has two kinds of needs:
– PHYSICAL – a human baby is born extremely fragile requiring physical care (feeding, hygiene, health, heat, tactile stimulation, etc.) without which he dies. The focus here is on what is done to the child.
-EMOCIONAL – Basic emotional need of the human being and without which it does not survive psychologically is the need for dependence, to count on each other. The human baby is born completely unprepared and will only be autonomous, with internal resources, after many years (in the middle class in our urban culture, only after adolescence). Here what matters is not having physical needs met, but how it is done.
In addition, the first stage of our life is pre-verbal and everything that happens to us depends on the verbal and emotional decoding of our mother / caregiver) . Without someone who can mirror our needs and emotions we have no way of knowing who we are. On the other hand how this person decodes our messages ends up constituting what we are, and it does so according to their own heritage of emotional experiences.
This first caregiver or caregivers work as a kind of relational bridge between the child and the world and take up, at first the place the “I” * child will take later. We are “WE” before being “I”, that is, the relationship we establish with our first caregivers, is the foundation stone of our identity (Erikson, E,:. 1976) and will also reflect our expectations of the world.
Abused children in these basic and fundamental care are like ticking time bomb for the future. The abuse reverberates throughout his personal and professional life.